In his paper the author then applied the above argument to the rest of Himsworth's contention, pointing out how any increase in the consumption of fat in Western nations must, for evolutionary reasons, have been small indeed by comparison with the increase in the consumption of sugar, this latter being of a magnitude to match the increase in the mortality of diabetes itself -- which, starting around the middle of the nineteenth century, progressed to such an extent that the disease, from being twenty-seventh in the list of causes of death in the statistics of the Metropolitan Life Insurance Company in 1900, became the third commonest cause by 1950. He also pointed out the relative rarity of diabetes in rural China and India, where most of the inhabitants do not yet show the food-sophistication exhibited by the West.
The author elaborated the whole of the above argument in a later work, on Peptic Ulcer (1962), [3] from which quotations will now be made, showing how certain objections that could be made to this line of reasoning may be overcome.
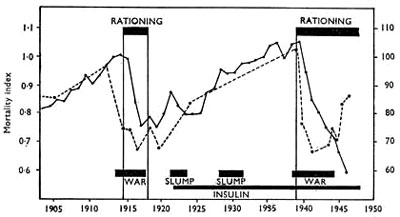
'As regards the decline in the incidence of diabetes during the war, the food shortage at that time caused a big fall in the consumption of fats and a corresponding rise in the consumption of carbohydrates. It is true that these latter were eaten relatively unrefined, mainly in the form of grain and potatoes and including little sugar, but since all the starch in carbohydrates is itself digested to, and absorbed as, sugar (glucose), it is clear that during the war the ultimate absorption of sugar in the belligerent peoples was higher than ever. How, therefore, can diabetes be related to the consumption of refined carbohydrates, especially sugar? Qualitative differences in sugar absorption were referred to in Chapter II and do not affect the present argument.
'Again, as regards the virtual absence of diabetes in primitive communities, these communities are usually ones that live almost entirely on carbohydrates, such as various grains and tubers. It is true that the carbohydrates are eaten substantially unrefined, as in the form of whole maize or millet, or home-pounded rice, but again, since all the starch contained in these is digested to, and absorbed as, sugar, it is clear that the ultimate sugar absorption in such communities, which do not eat refined carbohydrates, is higher than in civilized peoples, who do.
* * *
'The best way to expose the fallacy in these arguments is to consider another condition altogether -- dental caries. It is accepted everywhere that this condition is related to the consumption of refined carbohydrates, especially sugar. During the last world war, for example, a big fall in the incidence of caries occurred in all the belligerent countries, pari passu with the fall in the consumption of these refined products; also, in communities all over the world caries is slight or absent until these products appear amongst them, a recent striking example of this being provided in the inhabitants of Tristan da Cunha.
'This overwhelming epidemiological evidence quite rightly ignores the fact that during the war the total carbohydrate consumption in the belligerent countries went up, and that amongst communities which get little or no caries the total carbohydrate consumption is nearly always much higher than amongst civilized peoples who get a great deal of it. For what matters in the production of caries is not the quantity of carbohydrates consumed, but the form in which they are consumed -- to be more accurate, whether they have been refined or not. A whole cartload of carbohydrates in the form of raw apples or sugar-beet, for example, would do the teeth nothing but good, whereas a few cases of refined, sweet biscuits, leaving a sticky residue around the teeth, could initiate the fermentative process responsible for decay and therefore do the teeth great harm.
* * *
'Exactly the same argument, though involving a different pathogenic mechanism, is applicable to the causation of diabetes. Here also what is concerned is not the quantity of carbohydrates consumed, but the form in which they are consumed, i.e., whether they have been refined or not. There are two ways in which the consumption of refined carbohydrates could strain the pancreas, and all other instruments of sugar metabolism present in the body, and lead to the development of diabetes.
- 'Direct over-consumption of these carbohydrates, through deception of the tongue and appetite, as already explained, the over-consumption being measured not simply by the total amount of carbohydrates consumed, but by the total amount consumed relative to the total amount needed (for conversion into heat and mechanical energy at that time).
- 'Another way is to assume that what strains the pancreas is what strains any other piece of apparatus -- not so much the total amount of work it is called upon to do, but the rate at which it is called upon to do it. In the case of eating potatoes, for example, the conversion of the starch into sugar, and the absorption of this sugar into the blood-stream, is a much slower and gentler process than the violent one that follows the eating of a piece of Brighton Rock, for example, or other mass of concentrated sugar.'
In this connexion D. G. Campbell (1971, in Diabetes, Proc. 7th Congress Internat. Diab. Fedn., page 328. Amsterdam: Excerpta Medica) has recently produced a series of blood-sugar curves, showing how violent is the rise after eating neat sugar, compared with the gentle undulations after eating the same calorific value of carbohydrate in the form of the natural apple and potato. Even peeling the potato, which brings it into the refined category, and which the present author has long maintained is the only reason why potatoes have acquired a bad reputation in obesity, as set out in the previous chapter, makes a noticeable difference in the blood-sugar curve.
It is thus easy to understand that in the belligerent peoples during the war, as in primitive communities today, the stresses imposed on the pancreas, in spite of a large consumption of unrefined carbohydrates, were much less than in Westernized peoples at the present time. These, taking some 5 oz. of refined sugar per head per day, can often consume in a matter of minutes material that, in its natural form (for example, some 2-1/2 lb. of sugar-beet or up to a score of ordinary apples), would normally be eaten over several hours.
* * *
It is seen, therefore that the two objections to the present conception, noted above, can be met, and if the present writer's labours have achieved anything of value in diabetes, it is the elucidation of the absolutely crucial distinction, in all epidemiological studies of the disease, between the consumption of refined and unrefined carbohydrates.
From these preliminary considerations it will be clear that the author holds that the cause of diabetes lies essentially in the consumption of refined carbohydrates, which imposes unnatural strains upon the pancreas, either through over-consumption, or through rapidity of consumption and absorption, or through both.
At this point the author must stress that this work is concerned with the evolutionary and epidemiological aspects of the conditions studied, not the pathological ones. He therefore has no intention of entering the ever-changing labyrinth constituted by the pathological aspects of the pancreatic strain just mentioned. It would seem, for example, that anti-insulin may be no more than a natural response of the body to free insulin in the blood, appearing after injections of this substance in the treatment of diabetes.
The author will endeavour to show later that the hereditary features of the disease, which are undoubted, do no more than reflect the inheritance of personal build, including that of the pancreas itself, rendering the persons concerned more vulnerable to the new environmental factor; and that these features in no sense indicate hereditary defect. In short, to use the previous commonplace expression, he will try to show that the body is not built wrongly, but is being used wrongly.
II. The Incubation Period in Diabetes
The incubation periods in the various manifestations of the saccharine disease have already been discussed (Chapter II), and before dealing with certain epidemiological features in diabetes it will be desirable to refer to the incubation period of this particular manifestation. In 1959 G. D. Campbell [4] showed that there seemed to be a remarkably uniform period in a population exposed to a diabetogenic factor in their midst, before the disease itself appears amongst them. This period was formulated as 'The Rule of Twenty Years'. The rule was first worked out in the case of the urban Zulu, with incrimination of sugar as the factor most likely to be involved, the data being published later in the South African Medical Journal, in 1960. [5]
The rule of 20 years has since been supported by other writers in other countries, as will be seen in the case of V. Albertsson in Iceland and A. M. Cohen in Israel.
If the present author were asked how he would reconcile a 20-year incubation period in diabetes with the rapid drop in mortality he has just shown as occurring during the sugar rationing of the last war, his reply would be as follows (and this indeed was given in the earlier joint work): What is involved here is a reduction in the final spill-over of accumulated pathology into the production of overt disease, when such accumulation can no longer be held latent by the body's efforts in compensation. If the cause is removed, this spill-over can be stopped at once, though the accumulated pathology remains and may spill over later, as the body's compensatory mechanism ages (just as occurs in some other diseases, such as cancer of the lung due to smoking). And if all this is true of supposed new cases of diabetes, it is also true of the mortality which actually occurred. For, as regards stages of development, death is to overt disease as overt disease is to latent disease.
It is important to add that an incubation period of 20 years in the case of diabetes makes it impossible to argue, as E. P. Joslin [6] does, against the consumption of sugar being a cause of diabetes because 'in the United States the consumption of sugar has been stationary in recent years, whereas diabetes has increased; and in certain other countries, where the consumption of sugar is high, the incidence of diabetes is relatively low'. Countries with a present high sugar consumption, of fairly recent origin, as in the case of developing countries, may face an outbreak of diabetes in 20 years' time. This, indeed, is exactly what is happening in the Canadian Eskimoes today. Joslin also supports his argument with figures of the mortality from diabetes. Now the rule of 20 years concerns incidence. If the rule concerned mortality, it might well have to be altered to a rule of 40 years, since it would depend on how long diabetics lived after their condition was diagnosed. And that, again, would depend on the efficacy of the treatment in the country concerned. Viewed against the background of the present rule, therefore, let alone its extension, the second part of Joslin's argument is seen to be just as assailable as the first part.
III. Racial Studies: Africa and India
In the previous joint work, already alluded to, the above view on the causation of diabetes was strongly supported by racial studies, including those carried out in Natal by Dr. G. D. Campbell, [7] aided by Dr. E. L. Batchelor, which showed, on the one hand, a very high incidence of the disease in a large number of the descendants of past immigrants from India (the 'Natal Indians' numbering some 400,000 persons) and, on the other hand, a very low incidence of the disease in native Africans, of the Zulu tribe, still living in the tribal manner on unrefined carbohydrates (largely maize). These incidences of diabetes were matched with studies in sugar consumption, which in the Natal Indians is very high, but which in the tribal Zulus has always been very low, though in recent years there has been a spectacular rise (for example, from 6 lb. per head per year in 1953 to 60 lb. in 1964). It is to be noted, however, that past incidences and past consumptions, when compared with present ones, are often the most revealing studies of all, and the full. value of these studies may have yet to be seen; as stated earlier, they invite pursuit, either in the joint work or in the original papers.
(It may be added parenthetically, for later reference, that Dr. Campbell's studies also showed that the fat consumption in the Natal Indians mainly consisted, not of animal fats, but of vegetable oils, largely unsaturated, and yet the incidence of coronary disease in these people is almost as striking as the incidence of diabetes.)
Meanwhile, the incidence of diabetes in India itself is far lower, as set out in the joint work, in keeping with a far lower sugar consumption, too (some 12 lb. per head per year, [8] against at least 60 lb. in the Natal Indians [9] ). It is also important that the incidence of diabetes in India is much higher in the southern parts, where the staple food is milled, white rice, than it is in the northern parts, where the staple food is unrefined wheat and maize. Indeed, as regards the latter areas, personal communications to the present author in 1964 from Dr. J. G. H. Shaw and Dr. T. C. Skinner, from Mission Hospitals at Peshawar and Jalalpur Jattan respectively, state that diabetes is rarely seen there amongst the country-dwellers living on these unrefined foods, the admission rate for diabetes at the latter hospital, for example, during 1957-71 averaging only 1 case per 1000 admissions. Meanwhile, in the town-dwellers in Chandigarh and Amritsar the incidence of diabetes is much higher -- but then the sugar consumption is higher, too, a suggested figure [10] for Chandigarh being up to 4 lb. a month, which is much above the national average. It may be added here that however possible it is to relate diabetes in India to the consumption of refined carbohydrates, notably milled, white rice, it is normally impossible to relate it to the consumption of fats, for the Indian Council of Medical Research [8] has shown that in the masses of India the fat consumption is only half that considered necessary for the preservation of health.
Before leaving the subject of diabetes in India, it is significant, with reference to the clinical association of the various manifestations of the saccharine disease with each other, that the regions of highest incidence of diabetes are also those of the highest incidence of peptic ulcer -- the so-called ulcer belt in the southern part of India, where, as just said, the staple diet is milled, white rice. This subject will be pursued in Chapter X, on peptic ulcer.
It is also important to add that obesity, so rare amongst the masses in India, is very common amongst the masses in the Natal Indians.
Finally, to refer back to the rarity of diabetes in Africans living tribally, which is everywhere admitted, the incidence of the disease in urban Africans is, by contrast, reaching equality with that in the whites, [11, 12] just as it already has done in the cousins of these Africans, the Negroes in the United States, [6] where the diet closely resembles that of the whites.
A further point, which is of the utmost importance, is that the Zulu and Pondo cane-cutters in Natal, who have always been allowed to chew as much sugar-cane as they please, have been shown to be singularly free from diabetes -- indeed in over 2000 of these cane-cutters tested by Dr. Campbell [7] and his colleagues, all that has been found is a trace of sugar in the urine in 3 of them, which supports the contention that the consumption of unrefined carbohydrates is as harmless as that of refined carbohydrates is dangerous, assuming the former are eaten by the indigenous inhabitants.
This observation from Natal is in striking agreement with a statement of F. G. Banting, co-discoverer of insulin, in the Edinburgh Medical Journal, vol. 36, of January, 1929: 'In 1924, while visiting Panama, I was told by Dr. Clarke, pathologist of the Ancon Hospital, that on examining 5000 men who were applying for work on construction of the Panama Canal he had only found reducing material in the urine in 2 cases. Neither of these cases proved to be diabetic. This is the more remarkable because a large percentage of the labourers were natives of Dominica, where a main article of diet was sugar-cane. From the time the children are weaned until they die they eat the sugar-cane. There are also wealthy Spaniards living in Panama who eat large quantities of refined cane sugar. Indeed much of their food is cooked in syrup. The incidence of diabetes amongst this class is surprisingly high.' [13] Dr. G. D. Campbell brought this valuable reference to light.
It should be added that the above cane-cutters in Natal are now receiving a supplementary ration of refined sugar, and it will be interesting to see if their incidence of diabetes changes in the future.
IV. Other Racial Studies in Diabetes
It will now be convenient to relate diabetes to the consumption of refined carbohydrates in some other communities and countries, to supplement those already quoted. Actually, the present author knows of no country where this relationship cannot be established, always assuming the following:
- The consumption of unrefined carbohydrates, such as sugarcane, must be carefully weeded out. The importance of this has already been shown.
- The incubation period must also be carefully allowed for, as already set out.
- The consumption of refined carbohydrates must embrace all types of these, including not only refined sugar, but also refined (white) flour, polished rice, and in some countries even manioc or cassava (tapioca). Malted liquors such as beer, and many native brews, must certainly also be included in the consumption of refined carbohydrates. For malt sugar is a particularly significant example of these foods, and the errors that occur if its consumption is disregarded are discussed in detail in Chapter VIII, on coronary disease. All refined carbohydrates are liable to be consumed in excess, as explained in Chapter I, and, since all are absorbed as monosaccharide sugars, are liable to affect the blood-sugar curve to an unnatural extent, either in height, or in speed of ascent, or in both. But, being unnaturally concentrated to a greater extent than any other refined carbohydrates, table sugar, whether white or brown (demerara), is always the most serious in the production of disease.
a. Trinidad
The importance of considering the consumption of all refined carbohydrates is well seen in the incidence of diabetes in Trinidad. Thus, T. Poon-King [14] and others have pointed out that the incidence of the disease in that island was 2.37 per cent in the East Indian inhabitants, but only 1.44 per cent in the Negro inhabitants. Yet the sugar consumption in the two groups was almost identical at 47-48 g. per day, so the difference in incidence could not be related to sugar consumption. However, if refined cereals are also considered, the picture changes at once, for the consumption of these shows an average figure of 379 g. for the East Indians but a figure of 287 g. in the Negroes. The present author was in Trinidad during the Second World War, and knows it well and the multiracial society of which it is composed. After reading the above Lancet paper, he took the opportunity to revisit the island and meet Dr. Poon-King, who afforded him great help in exploring the figures given in his article and in establishing the point now being made.
b. The Eskimoes
In the previous work implicating the saccharine disease, the present author considered the incidence of diabetes in Eskimoes was lower than would be expected from their exposure in recent times to refined carbohydrates,, and it was suggested that if this lower incidence became confirmed, it might be explained by their lesser liking for these foods, owing to the normal lack of them in their natural environment. Time has since shown, however, that this explanation is unnecessary, because the lower incidence of diabetes has not been confirmed. Indeed, with the greater availability of sugar and white flour, the consumption of the former substance amongst Canadian Eskimoes has now risen to over 100 lb. per head per year [15] and, with the expiring of the 20-year incubation period already discussed, diabetes [15] is now commonly occurring amongst them. The same is true of other manifestations of the saccharine disease, in these people, such as gall-stones, etc., already set out in Chapter II.
However, as regards the more remote Greenland Eskimoes, the situation is much the same as existed amongst their Canadian cousins a decade and more ago, the consumption of sugar being still very low and the incidence of diabetes correspondingly low, too. [16] But the sequence that has occurred amongst the Canadian Eskimoes appears only too likely to follow amongst the Greenland Eskimoes, in which case the same sequence in the two groups will not only be evidence of diabetes being a manifestation of the saccharine disease, but perhaps also the strongest of any such evidence that exists.
The author is particularly indebted to personal communications from Dr. O. Schaeffer of the Charles Camsell Hospital, Edmonton, Canada, and from Dr. H. O. Bang of the Aalborg Hospital North, Denmark, for many personal communications on the Canadian and Greenland Eskimoes respectively, on whom they have performed such valuable studies.
c. Cherokee Indians
Professor K. M. West and others, [17,18] of the University of Oklahoma, U.S.A., have made a study of diabetes in certain racial groups. These groups included natives of the working class in East Pakistan (now Bangladesh) and the Cherokee Indians of North Carolina, U.S.A. Both these groups are of interest, because in each group the diet consists mainly of carbohydrates, and refined carbohydrates at that, but whereas the carbohydrates in the former group consist mainly of rice, with very little sugar, the carbohydrates in the latter group consist mainly of white flour, with large amounts of sugar.
In these studies, in each case on about 500 subjects over the age of 30 years without known diabetes, and matched as closely as possible, the incidence of the disease, as based on arbitrary blood-sugar criteria, was 1.5 per cent in the East Pakistanis and 26 per cent in the Cherokees. This difference is supported clinically by the vastly greater number of cases sent to hospital in the latter group. In the previous joint work it was shown that hospital admissions for diabetes in India average about 1 per cent. A personal communication from R. Bokat (1965), Director of the U.S. Public Health Service Hospital at Cherokee, forwarded by Professor West, to whom the author is greatly indebted for many personal communications, shows that the admissions for diabetes there average 12 per cent. Incidentally, for adult admissions only, the average is about double this -- 25 per cent. The question of inbreeding as a factor in this very high incidence is under discussion.
To turn back now to the diets, though in the paper no breakdown is given of the carbohydrates consumed, which supply the bulk of the calories in each case, we may assume that, as the Cherokees are living in the United States, where sugar consumption exceeds 100 lb. per head per year, the difference in the consumption of this particular foodstuff by these two groups will be very great, as it has already been shown in Part III, above, that the average sugar consumption in India is only about 12 lb. per head per year. The difference in fat consumption will also be marked, but less so, and, as seen in Part III of this chapter, the difference here is largely due to a below-natural consumption in the East Pakistanis. Furthermore, any difference in fat consumption cannot explain a remarkable difference in the incidence of obesity in the two groups, which is so often associated with diabetes. For obesity is rare in the masses in East Pakistan, but extraordinarily common in the Cherokees. In the present conception the difference in sugar consumption explains the difference in incidence not only of the diabetes but also of the obesity.
Such, then, is the diabetes- and obesity-riddled state to which the spirited Red Indians of history and literature have been reduced by the exchange of a natural diet based on unaltered Indian corn (maize), plus game and fish, for the most unnatural alternative based largely on white flour and sugar.
d. Iceland
A little over a century ago proteins and fats were forming a high proportion of the diet of the Icelanders, and, as with the Eskimoes, diabetes was probably unknown. Thus, even in 1938 V. Jensson, Director of Public Health, stated: 'Diabetes is a very rare disease in Iceland, and it is an extraordinary occurrence for doctors to come across it' (quoted by Albertsson). [19]
Unfortunately, the present situation is very different. In 1850 proteins and fats formed 80-85 per cent of the national diet, [20] but with the replacement of these foods in later years by the refined carbohydrates (white flour and sugar) this figure was already reduced to 45 per cent in 1940, and today the sugar consumption in Iceland is that of the Westernized nations -- well over 100 lb. per head per year.
With this change in the diet diabetes has first emerged and finally even become prominent. This development can be shown to have occurred within the 20-year incubation period worked out by G. D. Campbell, as already described.
There should be added to the foregoing, from Albertsson's paper, that obesity, which was rarely seen in Iceland before the First World War, is now a common condition.
e. The Yemen
Perhaps the most striking of these aetiological studies, however, because of its thoroughness, has been A. M. Cohen's (1960) upon the Yemeni or 'Black Jews'. [21] These people moved to Israel from the Yemen, where they ate mainly fat and protein foods, and where their sugar intake was one of the lowest in the world. When they moved to Israel the most striking change in their diet was a marked increase in sugar consumption, and in a group of people in whom diabetes was unknown the incidence of the disease rose to that prevailing in Israel (which exceeds that in many Westernized countries). Similar findings were noted amongst Kurdish immigrants.
f. Islands in the Pacific
Similar evidence pointing to the consumption of refined carbohydrates in the aetiology of a rising incidence of diabetes is available from studies on the Australian aborigines; [22] on the primitive inhabitants of New Guinea; [23] and on the Polynesian inhabitants of Mabuig Island. [24] More recently this evidence has been extended for Polynesia. [25]
g. Westernized Nations
Turning now to the Westernized nations, we may say that sugar consumption is very high in all of them (e.g., England: 120 lb. per head per year, as shown in Chapter II), and that the incidence of diabetes is very high, too. Thus, the Birmingham Surveys on some 20,000 persons, whose ages approximated to the national average, showed an incidence of about 1 per cent of overt diabetes, and about another 5 per cent of latent diabetes (that is, where people have abnormal glucose-tolerance curves, or where they show these too readily under unfavourable conditions), in whom the conversion rate is expected to be high. The results of these surveys (which are still being followed up) were published in 1962 and 1963, [26, 27] and are not out of harmony with other, earlier surveys on white populations.
Owing to variations in the methods of blood-sugar testing, and especially owing to variations in the interpretations of results in these tests, it is not possible in a non-technical work like the present one to make a close comparison between these surveys and those in other racial studies, especially as the age structure, to which the incidence of diabetes is so closely linked, is often radically different, but it does seem that the Indians in Natal, and therefore potentially the Indians in India, are exceptionally vulnerable to the disease.
V. Hereditary Considerations in Diabetes
Since diabetes as a congenital abnormality virtually does not occur (and it will be shown shortly that even its occasional appearance in the first ten years of life does not invalidate this statement), and since in any case its incidence in many populations far exceeds the figure of 5 per 1000 which the author has already shown represents the upper limit of incidence in hereditary defects, he rejects unequivocally that diabetes is for practical purposes ever primarily caused by hereditary defect.
That there not uncommonly exists in people a personal make-up of the pancreas and related structures, which make-up is obviously hereditary and may have been magnified through an unfortunate marriage in the parents, and which now renders these people unduly vulnerable to a new factor in the environment, so that they acquire diabetes, is incontestable -- but this is utterly distinct from hereditary defect, as already explained in Chapter I.
In the author's opinion there is a grave danger at the present time, as pointed out in the earlier chapter, that the hereditary features in diabetes may distract attention from the external factor in the environment, which is the primary cause and the only thing that really matters. Apart from indicating the threat in certain types of marriage, and the need for special supervision in certain children (to shield them from the external factor), the attention should be riveted on the primary cause.
The report of the working party appointed by the College of General Practitioners [28] on the family history of diabetes seems to be entirely consistent with the view expressed above on the hereditary aspects of the disease. The more the genetic predisposing make-up becomes pronounced, the earlier the disease begins, in the presence of the external causative factor. Or, as stated in the summary of the report, 'only diabetes of early onset has a strong genetic background'.
Diabetes in the First Years of Life
It is considered here that diabetes as a truly congenital complaint for practical purposes does not occur, even in the low ranges of incidence shown to hold for all congenital abnormalities, but that it does occasionally occur in the first years of life is incontestable. This fact is by no means in conflict with the present conception.
Thus G. B. Winter and others, [29] of the Department of Children's Dentistry at the Eastman Dental Hospital, London, have recently shown that 'there seems little doubt that in this country local factors are all-important in the causation of rampant caries in the deciduous dentition, and that the factor principally involved is the prolonged sucking of sweetened feeding bottles, hollow feeders and dummies'. Similarly, A. J. Salter [30] has drawn attention to the cariogenic effect of feeding infants, often from birth, on dried milks to which large amounts of sugar are added before or during reconstitution; and E. M. Sefton and J. Fletcher [31] to similar effects from using sweetened dummies. To the teat in these latter a small container is attached, of about 6-ml. capacity, to be filled with honey, treacle, syrups, etc., and 'many cases have been recorded where, in association with such sweetened dummies, the teeth of children aged 9 months to 2 years have been totally destroyed in the course of a few months'. [32, 33] If these practices can materially affect the caries rate in the deciduous dentition, it is not hard to see that, in those rare cases where the pancreas is extremely vulnerable to the external factor, they can likewise produce diabetes.
Quite apart from the use of sweetened dummies, it is to be noted that cereals, usually sweetened, are nowadays commonly given even during the first few weeks of life. [34] It is also to be noted that when sugar is added to milk feeds it is nearly always sucrose that is added and not the natural milk sugar, lactose, which may also be of importance.
Owing to the wide-ranging nature of the present work, it is not possible here to distinguish other than quantitatively between juvenile and adult-onset diabetes. That is, from the aetiological point of view the two are assumed here to differ in degree, but not in kind, which also coincides with the author's own beliefs in the matter.
References
1. Himsworth, H. P. (1949), Proc. R. Soc. Med., 42, 3 323.
2. Cleave, T. L. (1956), J. R. Nav. Med. Serv., 42, No. 2, 55.
3. -- (1962), Peptic Ulcer, 142. Bristol: Wright. (U.S.A.: Williams & Wilkins Co., Baltimore.)
4. Campbell, G. D. (1959), Congr. Abstr., S. Afr. Med. Ass., East London, 45. Cape Town: South African Medical Association.
5. -- (1960), S. Afr. Med. J., 34, 332.
6. Joslin, E. P., Root, H. F., White, P., and Marble, A. (1959), The Treatment of Diabetes Mellitus, 10th ed. Philadelphia: Lea & Febiger.
7. Campbell, G. D. (1963), S. Afr. Med. J., 37, 1195.
8. Mitra, K. (1953), In Diet Surveys. Indian Council for Medical Research.
9. Walker, A. R. P., Holdsworth, C. M., and Walker, E. J. (1971), S. Afr. Med. J., 45, 516.
10. Berry, J. H. (1967), personal communication (8 May, 1967).
11. Seftel, H. C., Keeley, K. J., and Walker, A. R. P. (1963), S. Afr. Med. J., 37, 1213.
12. Jackson, W. P. U. (1963), Ibid., 37, 1220.
13. Banting, F. G. (1929), quoted by Campbell, G. D. (1966), Ibid., 40, No. 2, 21.
14. Poon-King, T., Henry, M. V., and Rampersad, F. (1968), Lancet, 1, 155.
15. Schaefer, O. (1971), Nutrition To-day, 6, No. 6, 8.
16. Bang, H. 0., Dyerberg, J., and Nielsen, A. B. (1971), Lancet, 1, 1143.
17. West, K. M., and Kalbfleisch, J. M. (1966), Diabetes, 15, 9.
18. Stein, J. R., West, K. M., Robby, J. M., Tirador, D. F., and McDonald, G. W. (1965), Archs. Intern. Med., 116, 842.
19. Albertsson, V. (1953), Diabetes, 2, 1184.
20. Steffensen, J. (1950), quoted by Albertsson, V., in reference 19.
21. Cohen, A. M. (1960), Israel Med. J., 19, 6137.
22. Cook, C. E. (1963), personal communication.
23. Campbell, C. H. (1963), personal communication.
24. Winterbottom, H. J. (1961), Med. J. Aust., 1, 780.
25. Prior, J. A. M., and Davidson, F. (1966), N. Z. Med. J., 65, 375.
26. College of General Practitioners (1962), Report of a Working Party appointed by, Brit. Med J., 1, 1498.
27. -- (1963), Report of a Working Party appointed by, Ibid., 2, 655.
28. -- (1965), Report of a Working Party appointed by, Ibid., 1, 960.
29. Winter, G. B., Hamilton, M. C., and James, P. M. C. (1966), Archs. Dis. Child., 41, 207.
30. Salter, A. J. (1965), Brit. Med. J., 1, 59.
31. Sefton, E. M., and Fletcher, J. (1962), Ibid., 2, 482.
32. Stephens, R. R. (1958), Practitioner, 180, 438.
33. James, P. M. C., and Parfitt, G. J. (1957), Brit. Dent. J., 103, 37.
34. Asher, P. (1968), Lancet, 1, 535.
Next chapter
Table of Contents
Back to the Small Farms Library Index