Physical, mental and moral deterioration
AFTER one has lived among the primitive racial stocks in different parts of the world and studied them in their isolation, few impressions can be more vivid than that of the absence of prisons and asylums. Few, if any, of the problems which confront modern civilization are more serious and disturbing than the progressive increase in the percentage of individuals with unsocial traits and a lack of irresponsibility.
Laird (1) has emphasized some phases of this in an article entitled, The Tail That Wags the Nation, in which he states: "The country's average level of general ability sinks lower with each generation. Should the ballot be restricted to citizens able to take care of themselves? One out of four cannot." He has illustrated the seriousness of this degeneration by presenting details as follows:
Although we might cite any one of nearly two dozen states, we will first mention Vermont by name because that is the place studied by the late Dr. Pearce Bailey. "It would be," he wrote, "safe to assume that there are at least 30 defectives per 1000 in Vermont of the eight-year-old mentality type, and 300 per 1000 of backward or retarded persons, persons of distinctly inferior intelligence. In other words, nearly one-third of the whole population of that state is of a type to require some supervision.
From a broad view of the problem of modern degeneration it will be helpful to note the observations by Tredgold (2) in mental deficiency. He states:
It is thus evident that the condition of mental deficiency, whilst presenting many interesting problems to the physician, the pathologist, and the psychologist, has also a much wider interest and importance. Since in Man the predominate feature is Mind, and since it is by its development and evolution that human progress has taken, and must take place, it is clear that the question of its disease, and particularly of its defect, is one of supreme importance to the statesman, the sociologist, the philosopher, and the whole community.
In connection with these investigations among primitive races it is interesting to note that the data are in complete harmony with the data which clinical pathologists, clinicians and anatomists have obtained in their study of the physical and structural characteristics of individuals who make up the deficiency groups. In discussing the problem of the significance of the shape of the palate, Tredgold (2) states:
Palate--The association of abnormalities of the palate with mental deficiency has long been recognized, and there is no doubt that it is one of the commonest malformations occurring in this condition. Many years ago Langdon Down drew attention to the subject, and more recently Clouston has recorded a large number of observations which show conclusively that, although deformed palates occur in the normal, they are far and away more frequent in neuropaths and the mentally defective. He states that deformed palates are present in 19 per cent of the ordinary population, 33 per cent of the insane, 55 per cent of criminals, but in no less than 61 per cent of idiots. Petersen, who has made a most exhaustive study of this question, and has compiled an elaborate classification of the various anomalies found palatal deformities present in no less than 82 per cent of aments, (mental defectives), in 76 per cent of epileptics, and in 80 per cent of the insane.
Probably every city in the United States has made special provision for both mentally deficient groups and unsocial individuals, either in special schools or in special classes. In Cleveland, we have had a large school devoted to the problems of the so-called pre-delinquent boys, of whom nearly all have been before the courts and are assigned to this institution because they are not well enough adjusted to be kept in their normal school environment. In discussing the characteristics of these boys with the principal of that school, I asked him what the probabilities were that many of these boys would finally become involved in crime. His comment was, in effect, that they were virtually in the vestibule of a penal institute, when judged by the experience of previous boys from that school.
In approaching a study of this group, it is helpful to observe the experience of the well-equipped institutions organized for the correction of the abnormal trend which characterizes these boys. In this connection, there is a helpful report by the United States Dept. of Labor, Publication No. 203, which gives the result of tracing the after careers of 621 boys who were in five of the best-known correctional institutions. It was found that 66 per cent had been arrested and 58 per cent convicted one or more times after having been paroled from the institution. It is apparent from data of this type that probably the forces that produce these abnormal expressions cause irreparable damage in the brain tissue. Practically all recent crime reports are recording an increase in juvenile crime. The Children's Bureau of the Dept. of Labor stated (Nov. 4, 1938): "that juvenile delinquency spurted during 1937 for the first time since 1930," but it cannot explain why until further study.
Reports to the bureau from 28 courts in 17 states and the District of Columbia showed that they handled 31,038 cases during 1937, an increase of 3,000 over 1936. The report showed that 44 per cent of the cases involved children between 14 and 15 years old; 22 per cent those between 12 and 13 years, and 10 per cent those between 10 and 11. Boys' cases comprised 8 5 per cent of the total.
As an approach to this problem I have made an examination of 189 boys in the Cleveland school for pre-delinquents. I gave particular attention to those physical signs of nutritional injury, which seemed to be definitely assigned to the formative period of the child. We endeavored to obtain detailed information relative to the family history and to the birth of the child. We were fortunate in having the assistance of the officers, and of a nurse in the dental service of the Health Department of the Board of Education, a nurse who made visits to the homes of many of these boys to obtain the information directly from the mothers.
In this group of boys, there were twenty-nine for whom I had not sufficient details to include their cases in the studies. Of the 189 in the group, there were only three with sufficiently normal dental arches to be classified as normal. Accordingly, 98.4 per cent proved to be individuals with more or less marked abnormality. Many of the faces were very badly deformed.
While often it will be difficult to place the responsibility entirely on either parent for the child's abnormal physical development, it is of interest to study the birth rank of these children. The average number of children in the families represented by these 160 children is 4.75. Of these, thirty-five, or 21.9 per cent, are first children in the families represented; thirteen, or 9.1 per cent, are only children; thirty-nine, or 24.4 per cent, are last children; and thirty-six or 22.5 per cent, are fifth children or later. Sixty-two, or 38.7 per cent, are either the first or last child. It will be seen from these data that the first or last child, or even a late child in a large family, tended to have a distinctly poorer chance than the intermediate children in the families in which these studies were made. Statistical data relating the age of the mother and father to prenatal deficiency of their offspring reveal that abnormally young parents have a much higher percentage of defective children than do those in the most favorable child-bearing period of life. The group at the Cleveland school included only those boys who have been before the courts because of more or less serious phases of delinquency. If they are in a considerable part the products of a defective society, it seems quite unfair that they should be held entirely responsible for that delinquency, which has put them in this institution. If they are destined for a penal institute in which they will be held entirely responsible for that abnormality which resulted in their misdemeanor, as has been the procedure in the past, are they receiving just consideration? Society may be justified in protecting itself from their misdeeds by placing restrictions about them, but it does not seem that society is justified in shifting the entire responsibility to the affected individuals.
Recent studies of the mental capacity of felons brought before the Common Pleas Court in Cleveland have shown that of 3,197 convicted felons examined in the medical clinic only 42.3 per cent were classified as normal. Fifty-five and nine-tenths per cent were classed as defective delinquents and only 1.8 per cent as insane. The outgrowth of this study has resulted in the drafting by the Cleveland Bar Association of a new criminal law for Ohio to be presented to the coming State Legislature. This bill provides for the creation of a new criminal class composed of what are called defective delinquents. This includes morons and others of abnormal mentality but not insane who commit felonies or misdemeanors. The purpose of this legislation is to afford special treatment for law violators falling within the new classification, making it possible to segregate delinquents in separate institutions. The Ohio law like that of most other states now recognizes only two types of criminals, sane and insane, and if not insane they must be punished.
It is proper that we should ask who is to blame for the abnormalities which render these young men incapable of making the necessary adaptation to our environment.
An important characteristic of the boys in the Cleveland school was their low intelligence. Practically all were recorded as retarded or mentally backward prior to their transfer to this institution.
It is important that we note the characteristics of groups that are similarly retarded, but who have not demonstrated sufficiently unsocial characters to have to be placed in the pre-delinquent groups. We shall recognize them as individuals who may never commit unsocial acts sufficient to get them into trouble, though they will doubtless continue in the group of mentally backward persons. Such a group is to be found in the Outwaithe School in Cleveland. The children in this school, which enrolls about one thousand students, were examined in order to ascertain whether there might be groups that are similarly afflicted physically. The school is distinctive because it has a very high percentage of children who are backward mentally. Many of these children have been concentrated there in order to bring them under the influence of special teachers. In an examination of a cross section of the children, almost all were found to have had distinct injury in the formative period, as evidenced by the changes in facial form. A preliminary survey of the backward children of this institution was made by having typical classes selected by an official of the school from ages ranging from eleven to seventeen. I examined the arches and made measurements of the head and face. With the assistance of the school nurse I obtained records of the other children in the families selected. This latter survey was supplemented by field work by the nurse. The intelligence quotients, as reported in the records, were also provided. In the twenty-nine individuals so studied, seven, or twenty-five per cent were first children; fourteen, or fifty per cent last children in the families. Only one individual was found with approximately normal dental arches, that is, approximately three per cent of the individuals. Twenty-eight children, or 97 per cent, had abnormality of one or both dental arches. These children were placed in this institution because they were backward mentally, although as a group they are comparable to the group studied in the Thomas A. Edison School, where the grouping was based on delinquent traits. A cursory examination was made by observing other pupils in this school in their classes and on the grounds. A large percentage of severe facial and dental arch deformities and a very high percentage with definite disturbances in facial growth were evident. These data are presented as applying to a group of individuals characterized by a disturbed mentality, to the extent that they were assigned to special classes for the mentally retarded. While the group constituting the school population at Outwaithe represented the relatively large group of pupils assigned to special classes for backward children and did not carry the stigmata of delinquency carried by those of the Thomas A. Edison School, both groups had many physical defects in common.
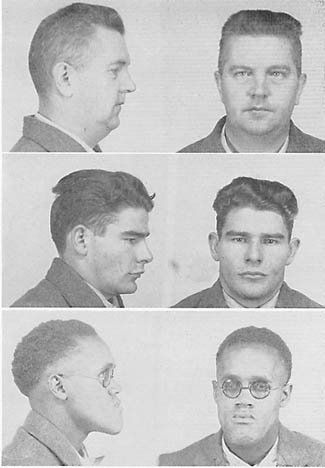
We are, accordingly, concerned with the relationship existing among various stages of mental backwardness, pre-delinquency and criminality. To throw light on this subject, I visited our State Penitentiary to observe the characteristics of facial and dental arch development of the individuals whose unsocial traits had brought them to this institution. I visited the dental clinic with the director, Dr. May, and saw the mouths of typical members of that colony as they were presented for oral examination. I asked the director what, if any, special features of the oral cavity he had observed to be characteristic of this group and different from those he had observed outside the institution in his private practice. He stated that he had noted continually that there was a tendency for the tongue to be too large for the mouth. This is a constant characteristic of another group of mentally injured, namely, the Mongoloid. This institution has a population of approximately four thousand individuals. A high percentage of them gave marked evidence of injury in the prenatal period as expressed in disturbances of facial form and the shape of the dental arches. In observing over half the population at work or exercise, I did not see one with a typically normal facial development. In Fig. 122 will be seen typical examples of this group. These show front and side views (see Hooton's recent book. 15a).
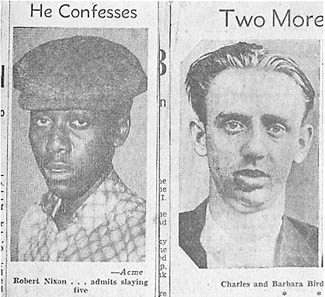
Newspaper daily illustrated reports of crimes committed by young criminals show almost continually these evidences of prenatal injury. Note the two characters Bird and Nixon, Fig. 123.
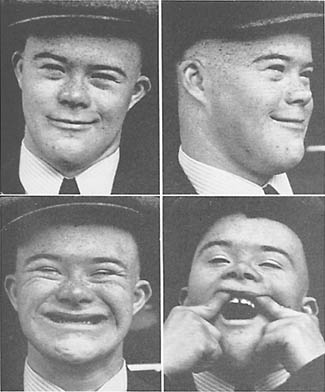
It is important to emphasize the fact that the disturbances in the development of the head, face and brain may have a variety of expressions. In the more severe form characteristic of the Mongoloid group, as seen in Fig. 124 the facial injury is typical and is associated with a mental disturbance which, in turn, has been shown to be associated with typical brain lesions. The individuals of that group, however, do not tend to be criminals. Indeed, their injury is too severe. As a group they are apt to be docile, tractable and happy. Indeed, in the mentally backward and criminal groups in their various stages, we find facial patterns typical of large numbers of individuals we see on the streets, who are in school or in business, and entirely capable of maintaining a respected and honorable position in society. Accordingly, it is not justified, and indeed would be entirely unfair, to associate their disturbed facial and dental arch development with traits that would be normally found in the grossly unsocial groups. We cannot by viewing the face evaluate the kind or extent of brain injury that is associated with prenatal malnutrition of that individual. Indeed, these various divergent facial patterns are accepted by our modern civilization as representative of the many varieties or patterns constituting a normal population. It is not until we see primitive groups living under a controlled natural environment that we see Nature's model and design of the human physiognomy.
We are concerned to know the percentage in any typical colony of our modern civilization that may be placed in the various classifications of normal, mildly backward mentally, severely backward mentally, unsocial, delinquent, criminal, idiots, epileptic and insane. Tredgold (2) reports two surveys in England and Wales which give figures on the proportion of the population that could be identified with definite lesions. It would be fortunate if a survey could be made in the United States that would indicate the extent of the increase in delinquents of various types, including racketeers and criminals. It would be very helpful if these data could be related to the degrees of prenatal injury. There are many phases of modern degeneration which lend themselves to study from the standpoint of the probable role of progressive decline in the efficiency of nutrition to the progressive increase in morbidity, mortality, mental deficiency and delinquency. This is discussed in the next chapter on Soil Depletion, Plant and Animal Deterioration.
From the point of view of this problem the differences between the modern white civilizations and many of the primitive groups is interesting. Criminal tendencies in isolated primitives are so slight that no prisons are required. I have referred to the Loetschental Valley in Switzerland, which, until recently, has been physically isolated from the process of modernization. For the two thousand inhabitants in that valley, there is no prison. In Uganda, Africa, the Ruanda tribes estimated to number two and a half millions, had no prisons.
Observation of Nature's normal facial patterns in the primitive racial stocks, establishes types within the limits of normality. The readers of this text by observing the individuals in any given families may see in how large a percentage of white families the progressive narrowing and lengthening of the face in the younger members of the family as compared with the older occurs. Further observations will enable one to recognize rapidly, even without experience and special training in anatomy, these evidences of prenatal injury.
I made a survey in the New England States, Quebec and Eastern Ontario, because the United States death rate from heart disease as reported by the American Heart Association was shown to be highest in Vermont and New Hampshire, followed closely by Massachusetts and New York. I first visited the New York State Hospital for tuberculosis patients at Raybrook, near Saranac. With the assistance of a member of the staff, I examined fifty young men and women in the wards. In that group, only three were found with normal facial and dental arch development. These three individuals were marble cutters who were suffering from silicosis. The forty-seven other individuals examined (94 per cent) were found to have marked evidence of injury in the developmental period. At the state fair at Rutland, Vermont, to which residents came from various communities throughout the state, I was able to count, by observing and recording the individuals who passed, that in each 100 people, three out of four gave evidence of injury in the developmental period. Similar studies were made at the State Farm for delinquent boys and girls, almost all of whom had been before the courts. 1 found that a very high percentage, approximating 100 per cent of those observed, had received injuries in the prenatal period. I then went to Quebec and studied groups of school children in the early teens. I observed groups in which a very high percentage gave marked evidence of prenatal injury. This seemed aggravated in districts where the farms had been abandoned, because the land was not producing as well as in the past. I studied Indians in two Indian Reservations, also, and there again found marked evidence of injury typical of our modernized communities. Similarly, a limestone district in Ontario was visited and critical observations were made of the facial form of the new generation, in regions in which the fertility of the soil had been definitely depleted through exhaustion. These again showed evidence of prenatal injury through faulty nutrition. The prisoners in a jail were examined, and all of them except two habitual drunkards showed marked evidence of prenatal injury.
If space permitted, it would be interesting to include here a discussion and illustrations of the physical characteristics of the racketeers and criminals whose pictures are shown in our newspapers almost daily. It is rare that a normal face is depicted in this group.
As an approach to more detailed study of the available information regarding the processes that are involved in the production of facial deformities, it will be helpful to think of the face as constituting the floor of the anterior part of the brain. The pituitary body is situated on the underside of the brain just back of the eyes. It is the governing body for the activity of growth, and largely controls the functioning of several of the other glands of internal secretion. It is, as it were, the master of the ship. We are, accordingly, primarily concerned with the role that it plays, and the forces which control its own development and function. Its dependence upon vitamin E has been demonstrated by many workers. For example, Dr. M. M. O. Barrie (3) has reported that an inadequate amount of vitamin E produces marked disturbance in the growth of the offspring of rats. He states:
The changes observed are similar in several ways to those produced by hypophysectomy (removal of pituitary gland). Marked degranulation of the anterior pituitary is found in both the abnormal young and the adult sterile animals. Lack of vitamin E therefore produces a virtual nutritional hypophysectomy in the young rat.
The work recently done in this field by Dr. Hector Mortimer and his associates in McGill University, Montreal, has included studies of skull development of rats. He has shown that the surgical removal of the pituitary body at the base of the brain in very young rats produces regularly a certain type of defect in skull development. This has been characterized by a lack of development forward of the muzzle or face, with a narrowing of the nose and dental arches. He found that by the addition of extracts made from the pituitary glands, which he had removed surgically, he entirely prevented the development of these defects, thereby establishing the relation of the injury to deficiencies of the hormones developed by that organ. Another approach to the problem on which he has expended much fruitful effort, has been in connection with the study of the skulls of individuals who are known to have disturbances in the functioning of the pituitary gland through the interference caused by tumors. Common illustrations are the cases of acromegaly or giantism. By associating these physical changes in bodily form with each x-ray, data obtained from skiagraphs, together with the history and the nature of the tumor, considerable information has been developed. Another important series of studies has included the correlation, by means of the x-rays, of the skulls of individuals suffering from certain types of physical and mental disturbances, with certain abnormalities in the skull as shown by the x-rays. By these various means Dr. Mortimer has been able to divide the various types of skull defects and developmental and growth defects into distinct classifications. With this yardstick he is able to classify individuals from their Roentgenograms. It is of interest that in his work, in association with Dr. G. Levine, Dr. A. W. Rowe and others at the Evans Memorial for Clinical Research and Neuro-Endocrine Research in Boston, important relationships have been established through the examination of over three thousand case histories. X-ray records of the skull are included in the studies. They report that independent and previous physiological investigations gave evidence at the time of the examination of disturbed pituitary function. Dr. Mortimer's excellent investigations seem to indicate clearly that facial and dental arch form are directly related to and controlled by the functioning of the pituitary body in the base of the brain. Dr. Barrie (3) reports that partial deficiency of vitamin E, as shown in the case of the female rat, results in the prolongation of gestation which may be continued as long as ten days beyond the normal period. The offspring under these conditions are abnormal. Further, animals deficient in vitamin E, occasionally give birth to a litter, but fail to lactate.
When we realize that one of the best sources of vitamin E is wheat germ, most of which is removed from white flour, usually along with four-fifths of the mineral, we see one cause of the tragedy that is overwhelming so many individuals in our modern civilization. In many individuals it may be wise to reinforce our modern white bread and starchy dietary with wheat germ, which can be obtained in package form from the manufacturers of flour. As this is put up in cans, all air is displaced with an inert gas when the cans are sealed. While in this way oxidation of the embryo which is very fragile, is prevented, as soon as the seal is broken, oxidation sets in and progresses rapidly, producing a product that is not comparable to the wheat embryo of freshly cracked whole wheat. My investigations indicate that Nature has put just the right amount of embryo in each grain of wheat to accompany that quantity of food. If the whole wheat is prepared and eaten promptly after grinding and exposing the embryo to oxidation, the effect desired by Nature is adequately provided.
It is important to emphasize in connection with the development of the deformities of the face that other skeletal deficiencies or abnormalities result from the same disturbing factors. One of these is the narrowing of the entire body, with a tendency to increase in height. This is shown in many of the family groups of modernized primitives. The effect of this narrowing of the body, which in girls results in the boyish type of figure due to the narrowing of the hips, introduces an entirely new and serious problem in the experience of our modern civilization when confronted with the problems of childbirth.
Among primitive races living in a primitive state childbirth was a very simple and rapid process, accompanied by little fear or apprehension; whereas, in the modernized descendants, even in the first and second generations of those individuals born to parents after they had adopted the foods of modern white civilizations, serious trouble was often experienced.
We have been considering the changes which take place in the skeletal growth as a result of the disturbances in the functioning of the pituitary body of the individual after birth, or of the mother during the prenatal period. We are also concerned with changes in the soft tissues, particularly the brain. I have presented data indicating that a very large percentage of mentally backward children have disturbances in facial development. The available data also indicate that a large percentage of those who are seriously injured in facial form have some disturbance in their mental or moral character. Whether there is relationship between the processes which develop these physical abnormalities in brain growth and mental efficiency, including emotional states and character traits is now to be considered.
An important contribution has been made to this phase of the problem by Dr. James Papez, Professor of Anatomy at Cornell University, (4) who concludes his report:
Is emotion a magic product, or is it a physiologic process which depends on an anatomic mechanism? . . . The evidence presented is . . . suggestive of such a mechanism as a unit within the larger architectural mosaic of the brain.
Research data have been presented which deal with the anatomical defects of the brain of individuals suffering from the typical mental and physical patterns of the so-called Mongolian idiot. In these cases the gyrus cinguli of the brain were found to be absent, which indicates the impossibility that these individuals function normally either physically or mentally.
Modern civilization has provided a large group of the defectives known as Mongolian idiots. They have very definite characteristics both physical and mental. Among the former, one of the most universal expressions is a vacant stare associated with a face that is markedly underdeveloped in the middle third, usually accompanied by narrow nostrils and a narrow upper dental arch.
One of the outstanding characteristics of the group is their inability to develop mentally beyond three to eight years of age. Because of the difficulty of building a character and intelligence level beyond infancy, these unfortunates are housed largely in state institutions for feebleminded. Since the physical picture is similar to that which occurs in a much less severe form in a large number of individuals in our modern civilization, it is important that we study this group in the light of the information that is available with regard to their physical, mental and moral characteristics, and in the light of such information as is available regarding their origin.
The surveys that have been made reveal the fact that nearly all of them are born to mothers more than forty years of age, and apparently at a period of very low efficiency in reproductive capacity. While most of the discussion and literature stress the importance of the age of the mother, some data are now available which throw responsibility also on the paternal side.
Korosi, as reported by Tredgold in Mental Deficiency, came to the conclusion as a result of the investigation of 24,000 unselected individuals that the children of fathers below twenty or above forty years of age are weaker than the children of fathers between these ages. Also, the children of mothers over forty years of age are weaker than those born to mothers below this age. Tredgold presents data connecting defective structures in the brain with certain phases of physical behavior and mental deficiencies. He quotes many authors whose data correspond with his own. Much of this material relates to accounts of incomplete prenatal development of nerve structures in the brain.
We are particularly interested in the origin and the nature of the brain lesions. Penrose, (5) in analyzing the relative etiologic importance of birth order and maternal age in Mongolism presents data obtained from an examination of 224 defectives in which the total number of children in all the families involved was 1,013. Accordingly, in these families approximately 20 per cent were so affected. The average number of children per family was five and one-half. He states:
Mongolian imbeciles are very often born last in a long family. This fact, which was pointed out many years ago by Shuttleworth, has led clinicians to believe that Mongolism is to some extent a product of the exhaustion of maternal reproductive powers due to frequent child bearing. . . . The conclusion is widely accepted with the reservation that the affected child is not necessarily born at the end of the family. Several cases are first-born, in fact, and it is sometimes stated that the conditions occur more frequently in first and last children than in other ordinal positions. There is, however, ample evidence that Mongolian imbeciles have a significantly later birth rank than normal children.
G. Ordahl (6) has reported on a study of ninety-one cases in which he found that fifty-six or 60 per cent were the last born. The families averaged five children. He states that "uterine exhaustion is the most commonly advanced reason for Mongolism." Madge T. Macklin (7) says, "It is usually stated that it (Mongolism) occurs more frequently in the later pregnancies owing either to reproductive exhaustion or to too advanced age of the mother." We are concerned at this point for evidence that will throw light on the relationship between the functioning of the pituitary body in the base of the brain and the development of this type of facial and mental deformity.
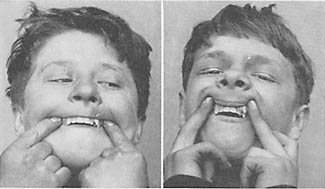
A striking case is that of a boy sixteen years of age who was a typical Mongolian idiot. He had two sisters who were much older than he. His mother was a partial invalid when he was born late in her life. We have no data relative to the details of the children who may have been lost. His father was living and well except for a railroad injury. This boy at the age of sixteen was infantile in many of his characteristics and developments. The genitals were those of a boy eight years old. The facial expression was that of the typical Mongolian idiot. By the Binet test he had a mentality of about four years. Roentgenograms of his hands showed that the epiphyseal bones had not united. He played on the floor with blocks and with rattles like a child. His interest was in children's activities. (Fig. 125.) The outstanding physical characteristic was his maxillary arch which was so much smaller than the mandibular arch that it went entirely inside it. In order to give him a masticating surface, and with the hope of helping him both physically and mentally, since several cases had greatly benefited by such an operation, I determined to widen his arch by moving the maxillary bones apart about one-half inch. The position of his teeth before the moving of the bones is shown in Fig. 126. Roentgenograms showing the opening of the median suture with increase of pressure are also shown in Fig. 126. An important phase of this case was that the left nostril was entirely occluded, and probably had been all his life. A rhinologist spent half an hour trying to shrink the tissue with adrenalin and cocain sufficiently to get air or water through, and was not able to do so. The quantity of air that he was able to inhale through his right nostril was so scant that he continually breathed with his mouth open. At night he was forced to lie with something like his coat rolled into a hard ridge and placed under the back of his neck and his head pushed far back to a position that would open his mouth and retain it so, or he would awaken, strangling because of the closing of his mouth.
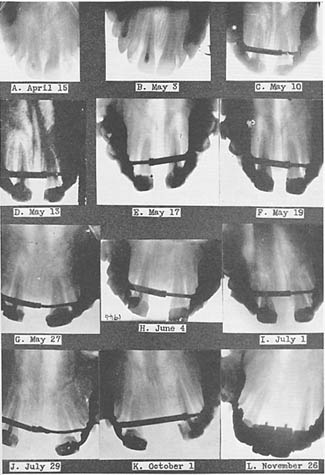
With the movement of the maxillary bones laterally, as shown progressively in Fig. 126, there was a very great change in his physical development and mentality. He grew three inches in about four months. His moustache started to grow immediately; and in twelve weeks' time the genitals developed from those of a child to those of a man, and with it a sense of modesty. His mental change was even more marked. The space between the maxillary bones was widened about one-half inch in about thirty days. This lateral pressure on the maxillary bones was accomplished by rigid attachments to the teeth of the two sides of the upper arch. The outward movement of the maxillary bones (which form the roof of the mouth and sides of the nose) by pressure on the temporal bones produced a tension downward on the floor of the anterior part of the brain, thus stimulating the pituitary gland in the base of the brain. In a few weeks' time he passed through stages that usually take several years. At first, he got behind the door to frighten us; later, he put bent pins on chairs to see us jump when we sat down, and finally he became the cause of a policeman's coming to the office from where he was conducting traffic on the corner below to find who it was squirting water on him when his back was turned. He developed a great fondness for calling people over the telephone, wanted to borrow my automobile to take his mother for a drive, and with his arm caressingly about the shoulders of one of the secretaries, invited her to go with him to a dance. All this change developed in about twelve weeks.
A most remarkable event happened in connection with this procedure. He lived in another city, and so, while with me, stayed in a boarding house at a little distance from my office in order that he might have frequent, and almost constant attention. On his return to his home town, his efficiency had increased to such an extent that his mother could send him with the money to the grocery store with the order for the day's groceries, and he could bring back the right change and could tell when it was correct. He could also come alone to me ninety miles by railroad and make two changes of trains and the various transfers on the street cars of the city with accuracy and safety.
He wore an appliance in his mouth to keep the bones in position. This appliance became dislodged; the maxillary bones settled together; immediately, or in a day or two, he lapsed into his old condition of lethargy accompanied by an old trouble, which had frequently been distressing, namely, nausea, this sometimes lasting for twenty-four hours. With the readaptation of the separating appliance and the reconstruction of the retaining appliance, he returned rapidly to his improved condition.
But a new problem had developed. We had changed an infant to a potential man with the impulses of a man, but with the mind of a child. With the change in his physical condition he became a menace in his community as a sex pervert. His mother died and his sister married. It became necessary to have him placed in a state institution for defectives. During the period he was in my care, he had learned to read child stories and newspaper headings, and had spent much time doing so. The changes in his physical appearance are shown in Fig. 125, above, front view, and below, side view. The first picture at the left shows his appearance before the operation; the second, thirty days after; and the last, six months later. The opening produced in the upper arch in front of half an inch was filled by supplying two teeth on a restoration, which at the same time held the maxillary bones in their new position. In six months he had developed whiskers and moustache. The progressive changes in the position of the maxillary bones with the opening of the median suture are shown in Fig. 126, together with the mechanical appliance. In the last view, the restoration carrying the porcelain teeth to fill the space is shown.
A very important contribution to our knowledge of the cause of Mongolism has recently been published by Dr. Clemens E. Benda, (8) Clinical Director of the Wrentham State School, Wrentham, Massachusetts, in association with the Harvard Medical School of Boston. He and his group have approached the problem of Mongolism from two different angles; first, as to determine whether it is accidental, and second, whether it is a unit of symptoms which can be related to more essential alteration. Their studies including careful anatomical studies have been made on the basis of an examination of 125 Mongoloids. He states:
Summarizing our investigations, the pituitary in mongoloids reveals a peculiar and definite pathology. On the basis of fourteen cases we feel justified in emphasizing that in mongolism definite failure of the pituitary development is to be found. Mongolism appears as a hypopituitarism of a specific type, in which the absence or deficiency of basophiles seems to be essential.
The evidence indicates that this severe type of facial and brain injury is related directly to a lowered reproductive capacity of the mother associated with age, since the majority are born to mothers beyond forty years of age, and to an inadequate nutrition of the mother, particularly in vitamin E since this vitamin plays so important a role in the nutrition of the pituitary body.
Important new data have been provided in an analysis of births in the United States in connection with the development of the Mongolian group. Bleyer (9) has reported a study of 2,822 cases. He reports that of the total births in the United States in 1934, of 1,095,939, there were 1,822 reported as Mongoloids. The average age of the mothers of these individuals was forty-one years. He reports data indicating that in the age group of mothers forty to forty-four the chances of the development of a Mongoloid would be seventy-five times as high as normal expectancy, and in the age forty-five to forty-nine the chances are 125 times normal expectancy. In a group of 1,942 Mongoloids, 1,100 or 57 per cent were last children. These data are in keeping with those of several other investigators, and emphasize the problem of depleted reproductive capacity.
The interesting problems involved in the birth of identical twins throw light on the origin of both physical and mental characters. It is a matter of great significance in connection with these studies that anomalies which we can associate with parental deficient nutrition are reproduced in both twins. Important additional light has been thrown on this phase by a family of six pairs of fraternal twins born to the same parents. These are reported by Dr. William W. Greulich, of New Haven. (10) It is significant that nine of these individuals (one of the oldest pair is deceased, and the youngest twins are yet babes in arms) show marked narrowing of the nostrils and lack of development of the middle third of the face, narrowing of the face and tendency to be mouth breathers. Further, the severity of this condition appears to be progressively more severe in the younger pairs of twins, sufficiently grown to show facial development. There is accordingly, evidence here of progressive lowering of reproductive efficiency, and the fact that both individuals are involved similarly has great significance, since they are fraternal twins arising from a single ovum. This seems clearly to relate this disturbance with a deficient germ plasm. Factors that are reproduced in identical twins would include both hereditary characters and those that are produced by a disturbance in environment resulting in an interference with normal hereditary processes. In a case of twins that are not identical, there is significance in the development of similar deformities which are likely to be of acquired origin rather than of hereditary origin. In Fig. 127 is seen a pair of twins. Note that they have similar disturbance in the development of the dental arches with the upper laterals depressed and the cuspids crowded outward in the arch.
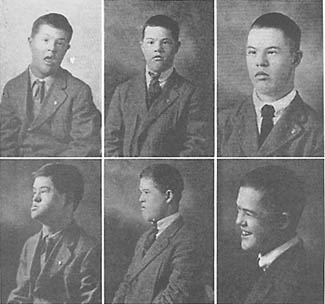
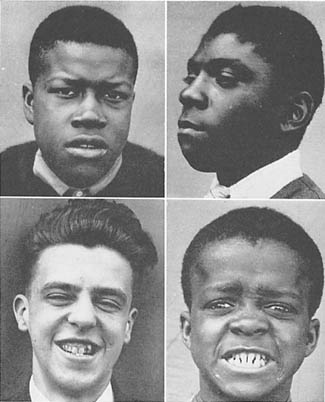
A very important source of information which deals with the relation of disturbances of the physical development of the head and mentality is provided by a study of the members of the teen-age group who are classed as mentally backward. In an examination of a Cleveland school in a colored district that has been set aside largely for boys and girls who are distinctly deficient in their ability to learn, it was disclosed that a very large percentage suffered from gross facial deformities when judged by these standards. Typical individuals in this group are shown in Fig. 128, one is white, lower left. It is clear that these boys were all physically injured in the formative period. Their clinical history indicates that the brain was involved in this disturbed development.
One of the problems involved in the development of the group of disturbances having physical and mental expressions, is associated with the sensitiveness of the body during the period of adolescence. Many students of degenerative problems have emphasized various phases of this large problem. Burt" commented: "It is almost as though crime were some contagious disease, to which the constitutionally susceptible were suddenly exposed at puberty, or to which puberty left them peculiarly prone." The age of adolescence is also the period of greatest susceptibility to dental caries. Data derived from chemical studies of the blood and saliva show that in this period of susceptibility to dental caries the supplies of minerals and vitamins are inadequate to meet Nature's demands, and the system borrows minerals from the skeleton to maintain vital processes. Lichtenstein and Brown (12) report data which reveal that educational quotients, like intelligence quotients, fall with increase in age during the years of developing puberty. They show that the educational quotient at nine years of age for the group studied was 100; at eleven years of age, 89; at twelve years, 83; and at thirteen years, 74. The changes in facial and dental arch form, which I have described at length in this volume, develop in this age period also, not as a result of faulty nutrition of the individual but as the result of distortions in the architectural design in the very early part of the formative period. Apparently, they are directly related to qualities in the germ plasm of one or both parents, which result from nutritional defects in the parent before the conception took place, or deficient nutrition of the mother in the early part of the formative period. Case records show that the first signs of delinquency generally make their appearance during these years. The age reported most frequently was that of thirteen.
One expression of the rate of the progressive degeneration that is taking place in the United States is the increase in delinquency and crime in young people between twelve and twenty years of age, as well as in crime in general. Edgar Hoover, Director of the Bureau of Investigation, has recently published data showing comparative figures for 1936 and 1937, during which time crimes in the United States increased from 1,333,526 to 1,415,816, an increase of six per cent. This increase is occurring in spite of the rapid development of social organizations for improving the environment.
Preventive measures among the unsocial group, who pass through the stages of predelinquency and crime, have been almost entirely confined to improvement in the social surroundings of the growing youth. While, no doubt, individuals with a low factor of safety are less likely to develop serious criminal tendencies under favorable environments, such factors as constitute a first-conditioning force, i.e., injury of the germ plasm, and deficient nutrition in the developmental period are not corrected by these efforts. These new data relating to the nature of the underlying causes strongly emphasize the need for beginning much earlier. Indeed, the preparation for the next generation should begin early in the life of the preceding generation.
Many investigators have emphasized the sensitiveness of the nervous system to disturbances in the formative period. Considerable data have been presented indicating that the tissues of the nervous system are the most easily affected of all the structures of the body. The extent of the injuries to the nervous system vary through a wide range.
Harris in his chapter on "Congenital Abnormalities of the Skeleton" in Blacker's (13) "Chances of Morbid Inheritance" has presented data indicating the sensitive period at which the ovum is most likely to be injured:
Few normal human embryos have been subjected to careful study. The vast majority of human embryos examined have been abnormal, and it is their abnormality which has led to their abortion between the sixth and thirteenth weeks of embryonic life, a critical period associated with the development of the placenta, during which the death rate is probably in the neighborhood of at least 15 per cent.
In tracing the development of the human embryo, he tells why the growth process is very different from that of the development of embryos of lower forms. He states regarding deformed ova: "Ova that survive the eighth week tend to live on to term, and are born as monsters." I have referred previously to a personal communication from Professor Shute, of the University of Western Ontario, which states that he had been impressed with the high percentage of deformities in aborted fetuses. This seems to be Nature's method of eliminating defective individuals. Harris says further:
It is sometimes suggested that threatened abortions in early pregnancy should not be treated by rest and quiet, as it is quite possible that the uterus is attempting to rid itself of a pathological ovum which might become a monster in the future.
The available data emphasize strongly that a very small percentage of the total gross deformities ever develop to menace society. Harris quotes Mall: (14)
He estimated from the records of 100,000 pregnancies that there were 80,572 normal births, 11,765 abortions of normal embryos and early monsters, and 615 monsters born at term. Thus at term 1 child in 132 is born with some anatomical defect. For each such case appearing at term, 12 others died and were aborted during pregnancy.
These data deal with gross defects involving physical deficiencies in the infant and indicate that the defects that are produced in the formative period, which are less severe than the above, are not recognizable at birth and may not be until long afterwards. According to Harris, "During the fourth week of embryonic life the head, brain and spinal cord are most susceptible to adverse conditions." He traces the sensitive areas of the various structures through the various weeks in the embryonic history. The deformities of the face among the primitive races which I have illustrated extensively frequently are not revealed until the eruption of the permanent dentition and the development of the adult features. While it is true that many children show deformity in facial development even in babyhood and childhood, those individuals are usually much more seriously injured when the adult face is developed.
Bloom (15) has presented the anatomical and histological characteristics of a defective born to a mother fifty-one years of age, whose general health was reported as good. The infant's facial pattern was markedly divergent from normal and practically no brain tissues had been formed. This expression of an extreme injury was entirely beyond that with which we are concerned in the study of the mental and the moral cripples who constitute an increasing part of our society. This is presented to emphasize Nature's inexorable requirement that each parent shall be individually physically fit for the responsibility of producing the next generation. Several primitive races studied have realized this responsibility.
There are some phases of modern physical degeneration in which most of us take part with remarkable complacency. We would consider it a great misfortune and disgrace to burn up the furniture in our homes to provide warmth, if fuel were available for the collection. This is precisely what we are doing with our skeletons by a process of borrowing, simply because we fail to provide new body repairing material each day in the food. You are all familiar with the tragic misfortune that overtakes so many elderly people through the accident of a broken hip or other fractured bone. Statistics show that approximately 50 per cent of fractured hips occurring in people beyond 65 years of age never unite. We look upon this as one of the inevitable consequences of advancing age. In Chapter 15 I have referred to the small boy whose leg was broken when he fell in a convulsion while walking across the kitchen floor. That bone did not break because the blow was hard but because the minerals had been borrowed from the inside by the blood stream in order to maintain an adequate amount of the minerals, chiefly calcium and phosphorus in the blood and body fluids. He had been borrowing from his skeleton for months because due to a lack of vitamins he could not absorb even the minerals that were present in the inadequate food that he was eating. The calcium and the phosphorus of the milk were in the skimmed milk that he was using but he needed the activators of the butter-fat in order to use the minerals. Simply replacing white bread with these activators and the normal minerals and vitamins of wheat immediately checked the convulsions.
We have many other expressions of this borrowing process. Much of what we have thought of as so-called pyorrhea in which the bone is progressively lost from around the teeth thus allowing them to loosen, constitutes one of the most common phases of the borrowing process. This tissue with its lowered defense rapidly becomes infected and we think of the process largely in terms of that infection. A part of the local process includes the deposit of so-called calculus and tartar about the teeth. These contain toxic substances which greatly irritate the flesh starting an inflammatory reaction. Many primitive peoples not only retain all of their teeth, many of them to an old age, but also have a healthy flesh supporting these teeth. This has occurred in spite of the fact that the primitives have not had dentists to remove the deposits and no means for doing so for themselves. Note particularly the teeth of the Eskimos. The teeth are often worn nearly to the gum line and yet the gum tissue has not receded. Many of these primitive groups were practically free from the affection which we have included in the general term of pyorrhea or gingivitis. Pyorrhea in the light of our newer knowledge is largely a nutritional problem. While nutrition alone often will not be adequate for correcting it, when established practically no treatment will be completely adequate without reinforcing the nutrition in so far as deficient nutrition has been a contributing factor. Nutrition plus the frequent removal of deposits, plus suitable medication will check and prevent pyorrhea but not correct the damage that has already been done. The elements that are chiefly needed in our nutrition are those that I have outlined as being particularly abundant in the menus as used by several of the primitive races. These are discussed in detail in Chapter 15.
Another important aspect of this problem of borrowing has to do with the progressive shrinking of the skeleton as evidenced by the shortening of the stature. I have measured many individuals who have lost from two to six inches in height in a decade or two. I have seen a few individuals who have lost as much as ten inches of their height by this process of borrowing from the skeleton. Our bodies need a certain amount of fresh minerals every day with which to manufacture blood. The days that these minerals are not provided in the foods they will be taken from our storage depots, the skeleton.
A particularly tragic phase of this problem of borrowing from the bone is seen in growing girls and is chiefly due to their ambition to avoid enlargement of their bodies to keep down their weight. The girls deprive themselves of body building material at a time when their bodies are growing and are requiring considerable new mineral. Forming bone has a prior claim on minerals, which is sufficiently commanding to induce the individual to borrow from bones that are already formed to provide for the necessary lengthening and growth. By this process many of the bones of the body are softened, particularly the bones of the spine. Curvatures develop, one of the expressions of which may be round or stooped shoulders.
Among primitive races this type of girl, so commonly seen in our modern civilization, is absent. Probably not one of these girls has ever suspected the suffering and sorrow that is being stored up for future life as a result of this bad management at a critical time in her development. Fig. 134 illustrates one of the tragedies of this borrowing process. Practically all of these physical evidences of degeneration can be prevented and fortunately many of them can be relieved in large part with an adequate nutrition. Even ununited fractures often can be induced to unite by an adequate reinforcement of the nutrition. This is true not only for young people but for elderly people as well.
In addition to the problems growing out of physical injuries through lack of development before birth, which express themselves as facial and other deformities, there is increasing need for concern for physical handicaps entailed in underdevelopment of the hips. The difficulty encountered at childbirth in our modern civilization has been emphasized by Dr. Kathleen Vaughan (16) of London. In her book, "Safe Childbirth," she states that faults of development more than race modify pelvic shape. In the Foreword to her book, Dr. Howard A. Kelly, Professor Emeritus of Gynaecological Surgery, Johns Hopkins University, says:
Dr. Vaughan presents such an array of facts and data that the book must impress every reader. It is of vital importance that her conclusions be considered, for in my opinion our methods of bringing up our girls and the habits of our women with many of the customs of 'civilized' life must be radically readjusted.
This important work should be made available for reference in the school libraries of the United States. Further data from it are presented in Chapter 21.
The great contrast in discomfort and length of time of the labor of modern mothers is to be contrasted with ease of childbirth among primitive mothers. Many workers among the primitive races have emphasized the vigorous health and excellence of the infant at birth. We have here, therefore, emphasis on the need in the interest of the infant that the mother shall have an easy and short labor. Both of these factors are directly influenced by the vitamin content of the mother's body as supplied by her nutrition and also by the physical development of her body if her mother at the time of gestation and prior to conception had adequate vitamins in her food to insure perfect germ cells.
The sensitivity of the brain to injury resulting from medication given the mother has been emphasized by Dr. Frederic Schreiber of Detroit. In his paper before the American Medical Association meeting in San Francisco, June, 1938, he was quoted as saying (17) that the analysis showed that 72 per cent of the children had shown difficulty in breathing at the time of birth or in the first few days following birth. He concluded, therefore, that this difficulty in breathing was the cause of the brain damage.
Difficulty in breathing would lead to a shortage of oxygen. An insufficient supply of oxygen in the blood stream would have serious effects upon the tissues of the brain. In this connection, he cited evidence found in post-mortem examinations that deficiency of oxygen caused microscopic changes in the brain.
X-ray photographs of some of the children examined by Dr. Schreiber showed various degrees of brain atrophy.
The contribution of Dr. Schreiber also emphasizes strongly the susceptibility of the brain tissue to injuries which may handicap the individual throughout life.
References
Next
Table of Contents
Back to the Small Farms Library