Chapter 10
Peptic Ulcer
PEPTIC ulcer is another condition that is considered here to be an unequivocal manifestation of the saccharine disease, and one that lends itself particularly well to the approach set out in Chapter I -- embracing the law of adaptation, and also the distinction between on the one hand bodily defect and on the other hand personal build reacting with a new environmental factor. This subject is dealt with very fully in a separate work, [1] but the main elements of the argument will be set out in this one (only the main references being given). Furthermore, certain rare forms of peptic ulcer such as occur after burns will not be included here, though they could easily be accommodated by the present conception.
I. The Prevailing Views on the Causation of Peptic Ulcer, Held Here to be Untenable
At the present time a widely held opinion on the aetiology of peptic ulcer incriminates the gastric (hydrochloric) acid as the primary cause. Now, though the virtual confinement of peptic ulcer to the stomach and duodenum, which are the only parts of the intestinal canal normally exposed to this acid, points to the acid as undoubtedly the agent involved in the production of ulcer, the law of adaptation excludes the acid altogether as a primary cause.
For this law indicates that the production of hydrochloric acid must be just as perfectly attuned to the requirements of the individual as is, for example, the power in his arms or his legs or any other part of his anatomy. Far from constituting a liability, the production of large amounts of acid in the stomach, passing under the term 'hyperchlorhydria', should be regarded as a most necessary asset. A powerful machine is useless unless it receives the right amount of fuel to run it. A powerful man is equally reduced to impotence unless his stomach produces the right quantity of acid to secure the digestion of the large amounts of food his energies require.
Yet, as stated above, opinion today is only too likely to exalt the hydrochloric acid to the status of a primary cause. Thus Illingworth: [2] 'The inescapable equation of ulcer aetiology -- acid-pepsin aggression versus mucosal defence -- allows for certain differences in the pathogenesis of duodenal and gastric ulcer. In duodenal-ulcer patients, gastric secretion is characteristically higher, the acid-bearing (fundic) area of the stomach larger, the gastric mucosa thicker, and the parietal-cell mass greater than is usual in normal people (Cox, 1952; Card and Marks, 1959). Gastric-ulcer patients, on the other hand, often have normal or subnormal secretion and atrophic mucosal changes. It is thus understandable that an increase in acid and pepsin should be incriminated as the dominant aetiological factor in duodenal ulcer, and impaired mucosal resistance as the underlying cause of gastric ulcer.'
The only chance of a statement like this not being in open conflict with the law of adaptation lies in the possibility of an excess of acid (hyperchlorhydria), or a deficiency of mucin, being a hereditary defect. And what does that chance amount to? In .the opening chapter we saw that no hereditary defect occurs more often than 5 times in 1000 births. Yet peptic ulcer is now so common in this country that about 10 per cent of men and 4 per cent of women develop clinical evidence of the disease at some time during their lives, the post-mortem evidence being nearer 20 per cent for each sex. [3] In short, the incidence of peptic ulcer is over 20 times as great as that of any known hereditary defect.
Also, the view that the hydrochloric acid is the primary cause of peptic ulceration is quite incompatible with the historical and racial incidence of the disease, for peptic ulcer was rare before the turn of the century, [1] and is absent in certain communities even today, as will be shown later.
Another opinion on the aetiology of peptic ulcer incriminates the 'stress' of living under modern conditions. But this cause is just as incompatible with the law of adaptation as was the preceding one. For what does evolution involve but a struggle for existence that has continued from the dawn of creation, and is still continuing? Such struggle for existence, with its ceaseless killing of one individual by another, represents the quintessence of stress.
Furthermore this cause, also, will be seen to be quite incompatible with the historical and racial incidence of the disease.
However, although stress here is absolutely excluded as a primary cause of peptic ulceration, it will be shown later that it plays a part as an aggravating factor. This aggravating factor consists of disregard of the instinct of appetite, in eating food that is not desired. In this connexion stress will be seen to be important -- but it can at once be nullified by attending to the instinct.
To sum up, as regards the causation of peptic ulcer, it is again considered that the body is not built wrongly, but is being used wrongly. And again the question is: in what manner is it being used wrongly?
II. The View Advanced Here on the Causation of Peptic Ulcer
Protein-stripping
In searching for a new environmental factor as the essential cause of peptic ulcer, it is necessary to refer again to 'the inescapable equation of ulcer aetiology -- acid-pepsin aggression versus mucosal defence', quoted earlier in this chapter. This equation has so dominated medical thought that a third factor has been lost sight of -- the natural defence against the hydrochloric acid provided by the buffering effect of the food. This third factor is of the greatest importance because, if the natural buffering by the food is reduced, and still more if it is removed altogether, it is clear that the mucous membranes are exposed to a much more serious attack from the acid than they are designed to support, and the whole of the above equation is upset. In this connexion it should be added that it is now known (as set out in the separate work) that the highest acidities in the stomach occur during digestion and not in the empty, resting state. Furthermore, the thin, distended wall of the stomach during digestion must operate against the mucosal defence, whereas the thick, non-distended wall in the resting state must operate in favour of that defence.
It is not difficult to see how, under modern food processing, this reduction in buffering power very easily occurs. For the only component of food that buffers the acid is the protein. Fats, starches, and sugars do not affect the acid at all. And in the refining of carbohydrates the protein is either seriously reduced or removed altogether. A little later it will be shown, in fact, that there is a remarkable correlation throughout the world between the consumption of these 'protein-stripped' carbohydrates and the incidence of peptic ulcer. Meanwhile, the extent to which the protein component is reduced, or altogether eliminated, in the refining of carbohydrates is shown in Table IV. [4]
|
Table IV -- Reduction or Elimination of the Protein Component in the Refining of Carbohydrates
|
|
Carbohydrate Foods
|
Processing Treatment
|
Percentage of Protein by Weight Removed in this Treatment
|
Protein Calories Present, as a Percentage of All Calories, Before this Treatment
|
Protein Calories Present, as a Percentage of All Calories, After this Treatment
|
| English wheat, wholemeal flour (100 per cent extraction) |
Milling and conversion to white flour (70 per cent extraction)
|
11.2 |
11.0 |
9.3 |
| Rice (husked only) |
Milling (70 per cent extraction) plus washing, plus boiling
|
30.0 (average) |
10.6 |
7.3 |
| Potatoes |
Peeling plus Boiling
|
Variable, about 4-16 per cent depending on the degree of slicing |
10.5 |
Variable; suggested figure 9.5 |
| Manioc tubers |
Peeling plus various water treatments
|
60.0 |
3.0 |
0.4 (tapioca) |
| Sugar-beet |
Extraction of refined (white or brown) sugar
|
100.0 |
12.0 (average) |
0.0 |
It will be noted in Table IV that the protein removed is estimated in protein calories as a percentage of all the calories present. This method of estimation is essential, but the reason will not be discussed here; it is dealt with in the main work.
Protein-displacement
It has already been shown in Chapter II how the concentration produced in carbohydrates during refinement leads to deception of the tongue and of the appetite -- and so produces over-consumption. This extra consumption tends to displace the consumption of other foods, which contain natural amounts of protein. In short, the refining of carbohydrate foods not only reduces the protein outright, but also leads to a marked increase in the consumption of these foods, so that to protein-stripping becomes added protein-displacement. Fig. 1 in Chapter II deserves re-scrutiny in this connexion.
Consequences of Protein-stripping and Protein-displacement
In Westernized countries like ours, where the total protein-consumption is high, neither of the above protein losses would probably have a serious effect on the neutralization of the gastric acid were it not for two other factors of great importance:
- The stripped foods are often consumed by themselves.
- The various parts of a meal largely remain distinct in the stomach.
1. As regards the first fact, consider any young couple in a cinema. In the middle of the performance they are only too likely to consume some sweetmeat, which will probably consist of almost pure sugar, with practically no protein at all. The calorific value of this sweetmeat is high and will result in a considerable secretion of gastric juice. The consequences will be that the membranes of the stomach and duodenum are exposed to almost completely unbuffered acid, often for several hours.
(Since these words were written, about 10 years ago, it is well known that there has been some fall in the incidence of peptic ulcer in this country, and that this fall has been chiefly in acute perforations. It is the author's deep conviction that such fall has been due to the large replacement of cinema attendances during this period by television-viewing in the home, where the consumption of concentrated sweetmeats is likely to be replaced by that of ordinary balanced meals. In this connexion it is of great importance that in this country during the last war, when exactly the same consumption of packaged sweetmeats took place in the shelters during air raids, a dramatic rise in acute perforations was recorded in almost all the cities involved; and this rise disappeared when sweet-rationing was introduced later. Those who find these facts hard to believe should consult the author's main work on Peptic Ulcer, where they are fully documented.)
Very similar events take place on other occasions, too, such as during 'elevenses', where some three hours after breakfast the almost empty stomach receives a cup of tea or coffee, often heavily sweetened with sugar but with very little milk, and therefore containing hardly any protein. Another example is provided by drinks of alcohol taken some time before meals, especially at cocktail parties. In all these cases the stomach is liable to be subjected to almost completely unbuffered acid, often for a long time. In civilized countries, therefore, there lies concealed, under the cloak of a respectable total protein protection, a protein protection that at certain times of the day is seriously deficient.
2. As regards the second fact, it cannot be argued that, where the protein calories have been heavily reduced in parts of a meal, though the total protein calories of the meal remain high, the same danger is not present. It may be very much present. Consider a meal where a glass of sherry (containing no protein calories) precedes a beefsteak, and a tinned fruit salad (containing only 1.5 per cent of protein calories) follows the steak. It cannot be argued that the gastric acid will be adequately neutralized in this meal, for the following considerations show that it will not.
In the first place, in any radiographic meal it is easy to see that every peristaltic wave carries some part of the meal straight into the duodenum. The first waves often fill the duodenal cap. It is not a fact that the stomach contents are churned up till an even mixture results, and then the pyloric valve is released and the whole meal projected onwards. In the second place, it has long been known to physiologists that the succeeding portions of a meal are arranged in corresponding layers in the stomach. [5] Nor does drinking affect these layers of food in the stomach, since fluids by-pass the food and leave the stomach almost immediately. Veterinary surgeons have discovered that all the above applies to animals, too. Fig. 10 shows this layering in the human stomach.

Fig. 10. -- Tracing from radiographs taken at the times stated after a normal subject had eaten 200 g. of fried meat ball without contrast medium, 50 g. mixed with neobar, and then 100 g. without. Tracing from Neilsen and Christiansen (1932). (Reproduced by kind permission.)
|
To sum up: there is obviously a fundamental difference in the protection afforded to the gastric membranes, by say, 12 oz. of protein food divided equally between three meals and the same 12 oz. divided between two meals with almost none in the third meal, as often happens in civilized countries today; and, if this fact is admitted, it is possible to extend it, through the known occurrence of layering, just described, to cover parts of meals. It may be added that the loss of buffering power produced by the removal of the protein element in carbohydrates can be, and has been, measured. [6]
The refining of carbohydrates has other serious repercussions on stomachic digestion. Thus, the removal of fibre lessens the mastication necessary in the food, and hence lessens, too, its impregnation with the alkaline, buffering saliva. This greater or lesser impregnation with saliva makes it impossible to go simply by the protein calories in foods, as is shown in the main work on Peptic Ulcer. Thus an apple with 3 per cent of protein calories may be much safer than chocolate with 4 per cent of protein calories. Furthermore, the absence of fibre alters the gastric emptying time, making it slower in the case of white bread [7] but much quicker in the case of sugary solutions. Such factors make it extremely unwise to regard any deviations from the natural process as not serious, especially since such deviations may be endlessly repeated. If Life has taught the author anything, it is the danger of trying to be clever at Nature's expense, as noted before in this work (see also Appendix).
Finally, it is not necessary to stipulate that the removal of protein leads to higher eventual levels of acidity in the stomach, for certain foods (including perhaps unrefined carbohydrates) may require for their digestion higher levels of acidity than others require (including perhaps refined carbohydrates). But what the removal of proteins certainly will do is to lead to these levels being reached in a quicker and more brutal manner which, though the mechanism involved is quite different, can impose strains on the defensive secretions of the stomach directly analogous to those produced by unnaturally concentrated carbohydrates on the insulin of the pancreas, as described in Chapter VII on diabetes. Furthermore, it is profoundly important, concerning this unnaturally rapid attainment of maximal acidities, that, as shown above, the stomachic contents enter the duodenum regularly all along the post-meal period, so that any insufficiently buffered acid strikes the duodenum right from the start.
III. Experimental Evidence
Supporting evidence for the foregoing has been published in a paper by J. E. Lennard-Jones, J. Fletcher, and D. G. Shaw [8] They showed in a series of test-meal studies that the climb in gastric acidity following the eating of refined-grain products is indeed considerably accelerated compared with that following the eating of their unrefined analogues. Their figure for this difference in the case of refined maize cornflour, as compared with whole-maize meal, is reproduced here (Fig. 11). This has a particular bearing as regards Africa, where so much maize is eaten. It is far the clearest of the present figures.
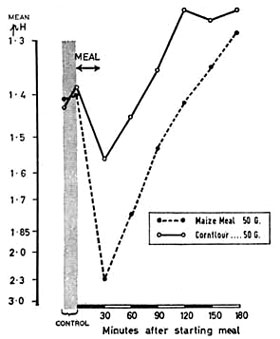
Fig. 11. -- Mean acidity of the gastric contents in 6 patients with duodenal ulcer after meals of whole maize and maize cornflour. (Reproduced by kind permission.)
|
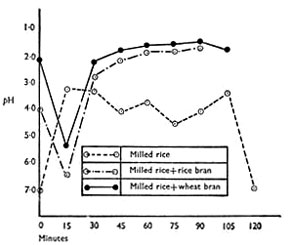
Fig. 12. -- Further studies in the buffering qualities of refined and unrefined carbohydrates. (By kind permission of Mr. F. L Tovey.)
|
Fig. 12 shows similar differences in early buffering in the case of rice with, and without, the addition of bran, for which the author is grateful to his friend, Mr. F. I. Tovey, whose buffering studies have been invaluable to him. [6] It will be noted that unlike the studies by J. E. Lennard-Jones and others, just quoted, these latter studies showed higher eventual levels of acidity in the presence of bran. This particular difference in results, however, does not affect the author's argument, which is not concerned with eventual heights of acidity, but with natural and unnatural speeds in the attainment of these heights. But there is a far deeper reason for this unconcern, which is that it follows, as an evolutionary axiom, that if a natural food, eaten with desire, generates a higher level of acidity, not only will this be harmless, but it should actually help the digestion of the natural food involved.
The author would like at this stage to present a small chart produced for him through the great kindness of Dr. John Temperley, now Consultant at the Preston Royal Infirmary, when he was working at University College Hospital some years ago (Fig. 13).
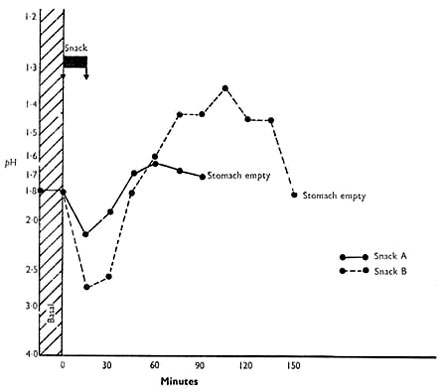
Fig. 13. -- Similar studies in a solution of sugars compared with raw apples. (By kind permission of Dr. John Temperley.)
|
Snack A: 'Hy-cal' (Beechams), 36.2 g., in water (67.5 cal., 126.7 g. H2O.
Snack B: 150 g. dessert apples, cored and quartered (67.5 cal., 126.7 g. H2O).
Graphs show pH of gastric contents after each meal. Mean of results in 4 patients with peptic ulceration.
It contrasts the average of the acid response in four subjects given a sugary (Beecham's Hy-cal) solution with the response when they were given an equi-caloric quantity of cut-up raw apple. It will be noted that the two curves are utterly different. At first sight it would appear that the natural carbohydrate inflicts greater acid strain on the stomach than the refined carbohydrate, though it has already been pointed out that for evolutionary reasons any height of acid following a natural food, eaten with desire, cannot be harmful. In this case, however, two things are to be noted: (a) the initial buffering referred to earlier is far greater in the case of the apple, and (b) the emptying time of the stomach with the sugary solution is little short of half that with the apple. Indeed Dr. Temperley told the author that the passage of such sugary solutions through the stomach is so rapid that it is often difficult to get out the gastric juice through the Ryle's tube to analyse the result.
Now the gastric acid is secreted at the fundic end of the stomach and is neutralized at the pyloric end and in the first part of the duodenum, where it meets the alkaline juices diffusing up from the second part of the duodenum. Therefore, with the above sugary solution there is not only much less time for the neutralizing mechanism to appear, but also much less time for it to act when it does appear. The completely different impregnation with saliva in the cases of the sugar solution and the apple is no doubt of great importance, too.
However, the author is convinced that the interference with the initial buffering is the main cause of the acid strain with the sugary solution. For according to McCance, [7] in the case of refined, white bread, the passage through the stomach is slower, not faster, than in the case of unrefined, wholemeal bread. The very rapid passage of sugar is presumably related to its ready solubility.
Meanwhile, the dangerous implications of sugar and sweets over the causation of peptic ulcer are obvious.
The author cannot agree with Mr. Tovey that a loss of some protective factor is involved in the causation of peptic ulcer by refined carbohydrates. The author believes that the causation normally lies directly in interference with the natural buffering of the hydrochloric acid, as set out above, and for the following reasons.
Firstly, the experience of the prisoners-of-war in Japan and elsewhere, many of whom are alive today, showed, as will be set out shortly, that the one thing the prisoners did not lack was fresh cabbage and other green vegetables, rich in such protective factors, which they grew for themselves. And yet the ulcer relationship to white rice was dramatic.
Secondly, assuming that careful attention is paid to the all-important dating of the observations (because of the stealthy spread almost everywhere of sugar, white flour, and white rice), the ulcer incidence all over the world can easily be related to interference with this buffering of the acidity through refining the carbohydrates. Especially is this true of the exceptionally high incidence of peptic ulcer where manioc (cassava) is eaten, where the incidence closely follows the varying interference with the protein buffer, dependent upon different modes of preparing different types of manioc, as will be described shortly.
Thirdly, peptic ulceration is confined to the stomach and duodenum, where hydrochloric acid is alone to be found. So it is simpler to deal with the acid and its neutralization than it is to introduce other factors. And the author is a strong believer in the empirical tendency of simple explanations to be correct explanations, as set out in the Preface.
Fourthly, Mr. Tovey attaches importance to the higher levels of acidity reached with certain natural foods -- which levels the author, for the evolutionary reasons carefully set out above, cannot regard as ever being harmful.
* * *
We now pass to the geographical incidence of peptic ulcer, and to the evidence from the prisoner-of-war camps in Japan and Russia, to show the relationship of the disease to the consumption of refined, protein-stripped carbohydrates.
IV. Geographical Incidence of Peptic Ulcer
This is too big a subject for the author to do more than touch on here, but a few of the more striking examples will be given. Details are set out in the separate work. However, he regards it as most important, in reading the following paragraphs, to remember that peptic ulcers occurring in undeveloped areas of the world, though not subjected perhaps to as complete a diagnostic investigation as in more developed countries, still cannot remain hidden indefinitely. They are certain to reveal their presence in the end, either by perforation, or by haemorrhage, or by scarring and obstruction. Therefore the evidence put forward by responsible medical officers in these areas should be given every consideration.
Two further points must be added. The first is that medical observations in the past are likely to be rendered more, not less, valuable by any difference in comparable observations today. This is largely because of the rapid and stealthy spread of refined carbohydrates in so many parts of the world. Indeed, Westernization throughout Africa is taking place so fast that the Hans Snyckers Institute has been set up at the University of Pretoria, Republic of South Africa, to record before it is too late the previous absence in Africa -- as established by earlier medical observers (including those still alive today) -- of certain disease conditions now increasingly appearing there. Such an institute is of great importance, for otherwise these earlier observations are only too likely to be written off as erroneous, whereas it is nearly always these observations that are the most revealing.
The second point is an evolutionary one. It may be advanced as axiomatic, from evolutionary considerations, that any foodstuff in its natural, unaltered state -- such as an unrefined grain, like the millet known as cholam, mentioned below -- which occurs in a person's natural environment and is eaten by him with relish, will not cause disease (including peptic ulceration). Therefore if, for example, eaters of natural cholam are getting peptic ulcer, then a personal glance at the larders in such sufferers' homes might be needed to exclude the presence of sugar, white rice, white flour, and even manioc (tapioca), to say nothing of fermented liquors. Such a glance might well explain why peptic ulcer has been observed in the eaters of cholam in India, whereas it has been conspicuously absent in the eaters of the parallel guinea-corn in Nigeria (see below ).
Africa
In Africa the incidence of peptic ulcer follows very closely the consumption of refined carbohydrates. Thus in the Charles Johnson Memorial Hospital, Nqutu, A. Barker reports 2 cases of peptic ulcer in 25,000 in-patients over 10 years (1950-60). These Africans subsist almost entirely on unrefined maize, as described in Chapter VII.
Similarly, in the heart of Ethiopia, where the natives live on unrefined teff (a form of millet), the government radiologist, M. Tausjo, reports that only 2 out of 1000 patients suffer from peptic ulcer, and that these are almost invariably those who have been eating Westernized foods. But the situation there may be very different today, and even in 1960 peptic ulcer was common in Addis Ababa and other large towns in Ethiopia, where white flour and sugar were being consumed in ever-increasing quantities. This evidence, and much other evidence of the rarity of peptic ulcer in the eaters of unrefined grains, is set out in detail in the main work on Peptic Ulcer. For example, in northern Nigeria where the main food is practically always the unrefined millet called guinea-corn (the equivalent of cholam in India), E. T. Mess (1960) reports 2 cases of peptic ulcer (both causing pyloric stenosis) in the Wusasa Hospital in 12 years.
Per contra, the disease is just as common in the Negroes in the U.S. Army as it is in the whites, [9] though formerly it was rare in U.S. Negroes when they ate hominy, made from unrefined maize. In many parts of civilized Africa the disease is very common, too. Thus, the disease occurs frequently, in typical form, in Kampala and Nairobi, where refined carbohydrates are commonly eaten by Africans. The disease is common in southern Nigeria, too, where the diet includes large amounts of manioc, which, as shown in Table IV, has lost a large amount of its original protein.
In Durban the incidence of peptic ulceration in the Zulus is still a long way behind that in the white residents (which may be explained by the diet being only semi-Westernized). In the Natal Indians, with their higher consumption of sugar, the incidence has already risen to equal that in the white residents.
India
In India peptic ulcer occurs only in certain regions, being absent in others. This ulcer belt is well known. Table V shows how closely the incidence of ulcer follows the consumption of refined carbohydrates. [10, 11] (It is to be noted that the milling of rice leads to a loss of about one-third of the protein, whereas hand-pounding the rice cuts out much of this loss.)
|
Table V
The Relationship Between the Incidence of Peptic Ulcer and the Consumption of Refined Rice
|
| State |
Population 1931
|
Number of Hospital Cases of Peptic Ulcer 1939
|
Incidence Per 100,000 of Population 1939
|
Percentage Rice-eaters Eating Milled Rice As Opposed to Home Pounded Rice 1940
|
| Bengal |
51,087,338 |
16,976 |
33 |
25 |
| Madras |
46,740,028 |
57,397 |
1143 |
70 |
| Bihar |
23,676,028 |
8,851 |
37 |
10 |
| Orissa |
18,653,555 |
4,132 |
29 |
20 |
| Punjab |
23,580,852 |
2,131 |
9 |
* |
| Assam |
9,247,857 |
926 |
10 |
15 |
| United Province |
49,614,833 |
4,460 |
11 |
15 |
| * Rice mostly replaced by unrefined wheat and maize. |
The fact that this table might be superseded today is not important. The rapid and stealthy spread of sugar, white rice, and even white flour might well make nonsense of it. What is important is that the table existed once and that it points to the evolutionary axiom given above: that natural grain, like any other natural food taken from a man's native environment, and eaten with desire, will not cause peptic ulcer; whereas refining the grain, or otherwise interfering with it, might well make it causative. Indeed, as stated earlier, before the author accepted any unrefined grain as a cause of peptic ulcer, he would want a search made of the sufferers' abodes to eliminate the presence of sugar, refined rice or flour, alcoholic beverages, or even bitter manioc. Too often he has found that local statements are very unreliable in this respect, especially perhaps amongst Indians, where such statements may have other objectives in view, and the great essay by Macaulay on Warren Hastings confirms his feelings about this. Too often there is given the inquirer an answer that he wants to hear. A native can have extraordinary prescience in this respect.
Peptic ulcer is commonest of all, however, in the southwestern parts of India, such as Kerala, where manioc is consumed in large amounts. As already stated, Table IV shows that this carbohydrate has undergone serious protein-stripping, and the subject will be further considered below.
It may be added that no relationship whatever exists between the incidence of peptic ulcer and the consumption of hot curries, [12] or between the incidence of the disease and any form of avitaminosis. [13]
Indonesia, Malaya, and China
In 1930 Kouwenaar showed by post-mortem examination that 151 ulcers and scars occurred in 1370 Chinese immigrants in Sumatra against only 8 in 1300 Javanese men. [14] It can be shown that these Chinese were eating milled rice, bought in the bazaars, whereas the Javanese were eating hand-pounded rice in their own homes. Yet peptic ulcer at this period of time was reported very rare indeed in the Chinese living in China itself, whenever they were eating home-pounded rice. [1]
Japan
In Japan the consumption of refined carbohydrates, in the form of milled rice and also considerable quantities of sugar, reaches a very high figure -- and the incidence of peptic ulcer is the highest in the world (34.7 per 100,000 as against 14.1 in England and Wales). [1]
V. A Note on Manioc Ulcer
Manioc (Cassava)
As the author has set down in his work on Peptic Ulcer, this potato-like plant is a native of South America, but in recent times has been introduced into other countries, such as India and Africa. It must also be stated that the tubers of most varieties of manioc (cassava) produce the highly poisonous prussic acid in their outer coat, as a protection against marauding insects. Therefore, before mankind can eat these tubers, he has to peel them, soak them (often after slicing) for a long time in water, and then throw the water away. This gets rid of the prussic acid, but the leaching also reduces the original 3 per cent of the protein calories to about 1.5 per cent. However, in the factories which process manioc to tapioca, the protein calories are reduced much more -- to 0.5 per cent, indeed, or even less. Since the natives eating manioc are amongst the poorest of the poor and often eat relatively little else, it is not surprising on the view advanced in this work, relating peptic ulcer to the removal of protein from natural foods, that this disease often becomes rampant amongst them. This is notoriously the case in Kerala in India, where manioc was introduced in the latter part of the nineteenth century, and where a very high incidence of the disease obtains. The Belgians likewise introduced manioc into Africa, first before 1920 and more extensively after 1940, and P. Konstam [12,13] has shown how closely, as regards manioc production and ulcer incidence, southern Nigeria in Africa resembles Kerala in India.
There is also a very high incidence of peptic ulcer in Burundi in Africa, where manioc is likewise widely cultivated, and where local opinion has related the high incidence to the big introduction of the plant there in the 1940s. This dating, however, could obviously apply to other possible causes too, but it does appear to the author as significant that the type of ulcer met is of the chronic sclerosing duodenal type, as occurs with manioc consumption, and not of the ordinary Western type, sometimes causing perforation. Another type of refined carbohydrate is commonly consumed in Burundi, too, and that is home-brewed alcoholic beverages, but the author cannot, himself, forsake the idea of a substantial manioc causation of ulcer there, as would be expected in a country that, with Rwanda, produced, at least in 1956, some 2 million tons of this dangerous foodstuff, which under natural conditions the tongue would not allow to be eaten at all. He is indebted for much information about peptic ulcer in Burundi to Mr. George Hamber, surgeon at the Hôpital de Buye, Ngozi, but he must stress that the opinions given here are his own responsibility.
* * *
Meanwhile, a further vital point may throw more light on this subject, for to the south, in Kalene, in Zambia, though manioc is to a great extent the staple diet, hardly any ulcer is seen at all. Before offering his own explanation of this remarkable fact the author must first express his deepest gratitude to Dr. D. Fitzgerald Moore, formerly Senior Medical Officer of the West African Medical Service, for certain key information on the subject of manioc; and to Dr. Evelyn Nightingale, recently of the Kalene Mission Hospital, Zambia, and to her assistant there, Miss Hilda Wadsworth, S.R.N., for details of the preparation of manioc carried out in Kalene.
Briefly, it may be stated that as well as the bitter, poisonous manioc, there is also a sweeter manioc that is only slightly poisonous or not poisonous at all. Whilst much leaching is needed for the bitter sort, little or no leaching is needed for the sweeter sort. Now in Burundi most manioc is of the bitter sort and the tubers are first peeled, sometimes cut up, and then soaked for several days in water. But in Kalene most manioc is of the sweeter sort, and here the tubers are soaked in water for several days before they are peeled. Both maniocs are then dried, pounded, and the flour added to boiling water to make a mush or porridge, all of which is eaten.
In this sequence one is powerfully reminded of S. T. Thomas's experience in India, set out on page 46 of the author's work on Peptic Ulcer, where in Orissa almost no cases of peptic ulcer come from the hills, where the water that the rice has been boiled in is drunk, whereas a great many cases of ulcer come from the plains, where the water is thrown away. And this water is rich in leached-out protein.
It may be added to the above that a careful analysis of the manioc mush or porridge at Kalene, by the Senior Public Analyst in Sussex, has shown that it contains 2 per cent of protein, and even more on a calorie basis, which is considerably above the percentages mentioned above for bitter manioc after treatment.
VI. Evidence from Prisoner-of-War Camps in the Far East, 1942-5
Interesting evidence on the aetiology of peptic ulcer is provided by data from the Japanese prisoner-of-war camps which, as far as the writer knows, has not been used in this connexion before. In these camps the commonest element in the diet was rice, and usually highly milled rice at that. When little other food was provided the diet approximated, therefore, to that already described for certain parts of India and Indonesia, and if the present argument is correct, peptic ulcer should have become conspicuous. Per contra, if the rice or other grain was not highly milled -- and sometimes it was not -- then the diet approximated to one of unrefined cereal, with very little animal protein, as already described for certain parts of Africa and Asia, and peptic ulcer should have become rare, no matter how reduced in amount the rest of the diet or how unfortunate the general conditions. The facts are as follows:
1. Singapore and Thailand (Siam)
Here the rice issued was highly milled but was supplemented by an issue of rice polishings until the end of 1943, when the issue ceased. In 1944 duodenal ulcer, which up to then had been infrequent, became, in the words of Julian Taylor's contribution to the History of the Second World War, 'a plague'. [1]
Meanwhile, it is a remarkable fact that among the prisoners of war taken away from Singapore in 1943 to work in Thailand on the tragic Burma Railway project, where the captives lost over 40 per cent of their numbers before returning to Singapore in 1944, peptic ulcer was almost never seen, and it is of the greatest interest that the rice issued to these prisoners was either unmilled, or supplemented with rice bran (normally used in Siam for feeding the pigs).
2. Hong Kong and Japan
In Hong Kong the prisoners were fed on milled rice and peptic ulcer symptoms and perforations were prominent. However, after two years a large proportion of the prisoners were transferred to Japan itself and here an important change occurred in the diet, the prisoners being given either a mixture of unmilled grains (including barley and millet), called the 'Korean mixture', or red (unmilled) rice. On this diet peptic ulcer symptoms and perforations, for practical purposes, vanished, no case being seen in Tokyo in some 6000 prisoners for over one year, and only I case being seen in Kobe and Osaka amongst 7000-8000 prisoners during the same period. [15] Meanwhile among the native Japanese population, which was largely fed on highly milled rice, the incidence of the disease quietly doubled.
Of one thing the medical officers were very confident: the dramatic improvement in ulcer symptoms and perforations in Japan, on the 'Korean mixture', was certainly not due to the appearance in the food of the C vitamin or other protective factor of this type. For in the Hong Kong camps there was never any lack of green vegetables, such as cabbage, which the medical officers, like the other prisoners, themselves helped to grow (largely assisted by the rather primitive drainage system present in these camps), whilst in Japan such green vegetables, though adequate, were, as the author's main work on Peptic Ulcer sets out, considerably reduced.
It may be added that during the above period Tokyo was almost completely destroyed by the U.S. B29's, and extensive damage was done to Kobe and Osaka. In the raids on London and other English cities a big rise in perforated ulcers occurred, [1, 16] as already described, which is in striking contrast to what happened in the Japanese camps. Quite clearly this difference cannot be explained by any form of stress argument.
The above key evidence from the Japanese prisoner-of-war camps was carefully recorded [15] by the author's brother, Surgeon-Captain H. L. Cleave, F.R.C.S., who was himself a prisoner and was in surgical charge of most of the prisoners, both in Hong Kong and Tokyo, and to whom the author is indebted for this and much other help in the preparation of the present volume.
3. Dutch East Indies
The Japanese prison camps in this area were investigated by a Dutch medical team in 1945-6, sent out by the Netherlands Red Cross, a full report of whose findings is published. In this report the rarity of peptic ulceration is noted -- these prisoners were nearly all fed on red, unmilled rice. [17]
It will be noticed that in spite of other variables in these camps, which tend to cancel each other out, the thread of relationship between the incidence of ulcer and the consumption of refined protein-stripped carbohydrates runs unbroken through all of them, just as it was shown to do in the preceding section on the geographical incidence.
Next chapter
Table of Contents
Back to the Small Farms Library Index
|
